KiwiRail track workers in a tunnel were caught out by a passenger train. They sprinted to escape. Everyone in a safety-critical role should be skilled at communicating clearly; making good decisions; working in teams; and situational awareness.
Executive summary Tuhinga whakarāpopoto


What happened
- At 1241 (times in this report are New Zealand Standard Time and are expressed in 24-hour mode) on Thursday 4 May 2023, a team of two KiwiRail track workers entered the rail corridor (for the purposes of this report, the term ‘rail corridor’ refers to anywhere within 5 metres (m) of the centre of the railway track) at Crofton Downs without permission and walked alongside the rail line towards tunnel 5 (the tunnel). On arrival at the northern end of the tunnel one of the track workers contacted train control (at the time of the incident, the national train control centre was located in Wellington Railway Station and was responsible for track authorisations and the safe movement of rail traffic throughout New Zealand) by telephone and requested time to conduct work on the Johnsonville line (JVL), stating their location to be at the 3.85 kilometre (km) mark (the JVL is measured by each kilometre starting at Wellington Railway Station (0 km). This increases in a northerly direction to Johnsonville (10.49 km). These measurements are referred to as kilometre marks) north of tunnel 5 and that they wanted to travel on foot through the tunnel to the south end. The tunnel is located between Wadestown and Crofton Downs.
- The train controller (the TC) went through their usual procedure for allocating track time and putting protection for the track workers in place before the track workers began making their way through the tunnel.
- However, the required protection from rail traffic, in the form of track signals being held at red (stop), was established by the TC at locations different from where the track workers were intending to work.
- As there was no protection in place at the correct locations, a Transdev passenger train entered the section of track that the track workers thought was blocked for their work.
- The two track workers were nearing the southern portal (the opening at each end of a tunnel) of the tunnel when they became aware of the Transdev passenger train entering the tunnel from the northern end. The track workers were able to exit the tunnel and move to a safe position before the train reached the southern portal.
- At 1248 the driver of the Transdev passenger train reported unexpectedly sighting the track workers to train control.
Why it happened
- The track workers arrived at the northern entrance to the tunnel without the required permission and without any protection from rail traffic.
- The TC recorded the intended track occupation on the train control diagram at locations different from those requested by the track worker and applied electronic blocking protection at those incorrect locations. The TC authorised the track occupancy to the track worker over the telephone rather than the radio.
- The track worker did not identify the location discrepancy while listening to the TC state the protection details and repeated back the incorrect locations without challenge.
What we can learn
- All personnel undertaking safety-critical roles should adhere to the principles underlying the application of non-technical skills to ensure that they share the same mental models and have a clear understanding of what is required of themselves and others to complete tasks safely.
Who may benefit
- Rail operators (including train controllers), rail protection officers and track maintenance personnel may all benefit from the findings in this report.
Factual information Pārongo pono
Narrative
- From 26 April until 4 May 2023, passenger rail operations were disrupted in the Wellington region because of operational issues with KiwiRail’s track evaluation car.
- This led to the implementation of temporary speed restrictions for trains, causing a reduction in the number of passenger services running daily and cancellation of some services.
- During this period, train controllers tasked in the Wellington metropolitan passenger train control area experienced an unusually low workload in comparison to their normal activity.
- On 4 May 2023 the issue with the track evaluation car was resolved and rail services returned to normal operations.
- The day before this, at 1214 on 3 May 2023, train control received a slip-detector8 alarm activation on the JVL at the 2.44 km mark.
- Slip detectors are placed at strategic locations on KiwiRail’s network to provide early warning to train controllers that an area of line may be compromised by slip debris.
- On receipt of the alarm, the on-duty train controller followed KiwiRail procedure, initiating a speed restriction for rail traffic, annotating the train control diagram and arranging for the area of line to be inspected.
- As there was reduced rail traffic at the time, an inspection team rode on a Transdev passenger train later that day to view the site of the alarm activation. No slip debris was observed by the inspection team and trains were authorised to pass through the area at a reduced speed of 25 kilometres per hour (km/h) until the slip alarm could be reset.
- Resetting the slip alarm required physical access to the rail-side equipment. To avoid further disruption to the rail schedule, the infrastructure team planned to reset the slip alarm after the passage of the final scheduled train for that day.
- Between 0145 and 0330 on 4 May, the infrastructure team inspected the JVL while they travelled by hi-rail vehicle9 to the slip-detector location at the 2.44 km mark to reset the equipment. Once this was done, they advised train control that the JVL was cleared for normal line speed.
- At about 0330 the train controller acknowledged this authorisation and made the necessary annotations on the train control diagram.
- At 0530 the TC, who was the day-shift train controller, started their shift on the Wellington metropolitan desk after receiving a handover from the night-shift train controller. Part of the handover process involved reading and understanding the information recorded on the train control diagram.
- At 0538 the driver of the first northbound JVL Transdev passenger train of the morning contacted train control to advise that a train stop trip (TST) (see Figure 3) had been activated between tunnels 4 and 5 and gave the location as “south of tunnel 5”.

- The TST location south of tunnel 5 corresponded with a build-up of loose rockfall at the 3.567km mark (see Figure 4).

- The TC recorded the TST activation by marking “Trip #5 tunnel sth” on the train control diagram at the same location that the slip alarm was activated the previous day, although the two alarms were in fact activated at different locations – the slip alarm at the 2.44 km mark between Wellington and Wadestown, and the TST alarm at the 3.567 km mark between Wadestown and Crofton Downs (see Figure 5).
- An hour later at about 0638 a second driver reported that the TST had been activated on their train at the same location, south of tunnel 5.
- On receiving this information, the TC notified operations support (a help desk referred to within KiwiRail as 155). The help desk tried to call out members of the infrastructure team to attend the TST activation site but could not contact them.
- At 0640, after receiving no response from the infrastructure team, 155 sent text messages to the infrastructure supervisor and field production manager but did not receive any response.
- As the fault had not been attended to it remained active in KiwiRail’s fault logging system.
- No further action was taken by 155, and there were no further reports of trains encountering TST activations that morning.
- At about 1100 the infrastructure supervisor read the text message sent earlier by 155 and began to arrange for the fault to be inspected.
- The infrastructure supervisor assigned a track worker (TW1) to inspect the track at the TST activation site, reported by 155 to be at approximately the 3.533 km mark on the JVL.
- TW1 arranged for another track worker (TW2) to assist and they both left the Wellington yard, travelling by road in a KiwiRail service truck towards Ngaio station.
- On arrival at Ngaio station the track workers realised they would not be able to access the alarm site from there and continued driving to Crofton Downs station, approximately 1 km north of the tunnel.
- At Crofton Downs, TW1 confirmed they were at the closest access point to the reported alarm site by checking a track metrage sign.11
- The two track workers collected shovels and a Mis 71 pad12 from the truck before waiting for a southbound passenger train to depart Crofton Downs station.
- Once the southbound train had departed, the two track workers made their way to the side of the track and walked along an access path beside the railway line for about a kilometre before arriving at the northern portal of the tunnel (see Figure 5).
- This access path was for maintenance purposes only, and the track workers should have obtained permission before its use to ensure that protection from rail traffic was established.
- At about 1240 TW1, who was not carrying a portable radio, contacted train control using a personal mobile phone and requested track time to walk through the tunnel to the alarm site.

- TW1 gave the TC the location as being at the 3.85 km mark, north of tunnel 5. This location was between Wadestown and Crofton Downs (see Figure 6).
- The TC applied electronic blocking by first ensuring that the required signals were at red (stop), then moved the cursor on the mimic screen14 over each signal before right-clicking on the signal and activating a block command through the train control system. This ensured that the signals could not be changed to either green or yellow (proceed) without removing the blocking. Before removing any blocking from the signals, the TC had to conduct a series of checks, including ensuring that all workers were clear of the area.
- The TC advised TW1 that they had permission to work between the 3.85 km mark and Wellington, and that blocking had been applied between 97 signal Wellington and 4L signal Wadestown (see Figure 6). TW1 was given a start time of 1243 and was to be clear of the track by 1248 (five minutes later).

- TW1 repeated this information back to the TC while filling out the Mis 71 form.
- The blocking established by the TC (between 97 signal Wellington and 4L signal Wadestown) was incorrect. It did not prevent rail traffic from entering the section of track in which TW1 and TW2 were working.
- The correct blocking should have been between 8R A and B signals Wadestown and 4L A and B signals Ngaio (see Figure 6).
- Neither the TC nor TW1 identified during the telephone conversation that the blocking locations were incorrect. This is discussed further in the analysis section (see also para 2.66).
- On completion of the telephone call, TW1 and TW2 began jogging through the tunnel from the north end towards the south end. They only had five minutes of track time originally allocated, which by the end of the call effectively left only four minutes remaining. The tunnel was 127 m long and curved to the right in the direction the track workers were moving.
- TW1 was in front using the flashlight function of their mobile phone to illuminate the path as there was no form of internal lighting within the tunnel and the track workers did not have torches with them.
- As they jogged through the tunnel, TW2 heard the sound of train wheels and saw light appearing on the tunnel walls coming from behind them. TW2 called out to TW1 and the pair began running faster towards the southern portal.
- The pair exited the south end of the tunnel and immediately moved to a safe distance from the track on the eastern side of the portal (see Figure 1).
- Transdev passenger train TDW9237 exited the tunnel about 5 seconds after the track workers had reached a place of safety.
- At 1248, TW1 contacted train control by telephone to rescind the blocking protection. No mention of the near miss with the train was made during this call.
- The driver of the train was concerned that they had not known about the track workers on the JVL and, knowing that other trains were in the area, contacted train control by radio to report the location of the track workers.
- On receiving this information, the TC rechecked the train control diagram against the known location of the track workers and realised that protection had been put in place to cover the site of the earlier slip detector alarm at the 2.44 km mark, and not the TST activation site at the 3.567 km mark.
- The TC immediately reported this to their supervisor, who remained with the TC while they investigated what had happened.
- Meanwhile, the two track workers, remaining clear of the track, had walked to the site of the loose rockfall, about 60 m further south of the tunnel’s southern portal.
- At about 1252, TW1 called train control and requested further track time to clear the rockfall that had caused the earlier TST activations.
- The TC, under supervisor observation, established protection for the track workers at the correct location to carry out the clearing of the rockfall.
- The supervisor informed the Network Control Manager (NCM) of the potential safe-working irregularity and the NCM remained near the train control desk while the circumstances of the incident were being investigated.
- At the end of their allotted track time, TW1 called train control to advise that the work was complete and that blocking could be removed. The NCM then advised TW1 that an irregularity had occurred and that TW1 should contact their line manager.
- TW1 attempted to contact their line manager by telephone but was unsuccessful as the manager had completed an overnight shift that morning and had not yet returned to work.
- Meanwhile, the NCM had replaced the TC involved in the incident with a relief train controller who continued working the Wellington metropolitan train control area.
- At this stage, TW1 and TW2 were still at the southern end of the tunnel and needed to walk back through the tunnel to return to their vehicle parked at Crofton Downs.
- At 1316 TW1 contacted train control for permission to walk back through the tunnel. This permission was approved and the trackworkers were allocated time to walk back through the tunnel and return to their vehicle.
- On returning to the vehicle, TW1 was contacted by their line manager who advised the track workers to return to the depot in Kaiwharawhara.
- TW1 drove the vehicle 4 kilometres to the depot, whereupon both track workers were required to undergo post-incident drug and alcohol testing.
Personnel information
- TW1 had three years’ experience as a track worker, held all the required current competencies for the role and was qualified to establish track protection. On the day of the incident, TW1 was the senior track worker within the team as the qualified supervisors were off shift. TW1 underwent post-incident drug and alcohol testing and provided a non-negative16 (failed) result. Further laboratory analysis confirmed the initial result as a positive (failed) test.
- TW2 had one years’ experience as a track worker and held all the required current competencies for the role. TW2 underwent post-incident drug and alcohol testing and provided a negative (passed) result.
- The TC had 19 years’ experience as both a signaller and train controller. They held all the required current competencies for the role. The TC underwent post-incident drug and alcohol testing and provided a negative (passed) result.
Meteorological information
- The weather at the time of the incident was inclement. It was raining heavily with a temperature of 17 OC.
Recorded data
- The Commission obtained CCT (Closed-circuit television) footage and Tranzlog data for TDW9237 from Transdev.
Site information
- Tunnel 5 is a 127 m curved tunnel located between the 3.633 km mark and the 3.76 km mark on the JVL. Stations either side of the tunnel are Crofton Downs and Wadestown. The tunnel has no road access, but there is a walkable access track for KiwiRail personnel that runs alongside the rail line from Crofton Downs to the northern portal.
Medical information
- Laboratory testing confirmed the presence of tetrahydrocannabinol (THC) in TW1’s sample. The pattern of THC consumption and recency of use, and therefore the level of THC impairment, was not determined by a secondary test as TW1 left KiwiRail’s employment immediately. As the level of impairment was not established, no determination could be made as to whether THC impairment was a factor in this incident. This is discussed further in the analysis section (see paras 3.29–3.31).
Survival aspects
- Both track workers were able to reach the southern portal and a place of safety before the train reached their location. There was a refuge bay inside the tunnel that may have accommodated both workers if required. Had one or both of the workers not been able to reach either the refuge bay or portal they could have been fatally injured had they been struck by the train.
Previous occurrences
- On 24 March 2019 a rail protection officer conducting protection duties in Westfield yard lost situational awareness and allowed a signals technician into a work area without the knowledge of train control. Subsequently electronic protection was removed by train control while the signals technician was still conducting work (Rail inquiry RO-2019-101 Safe Working Occurrence, Westfield yard 24 March 2019, Transport Accident Investigation Commission, April 2020). The key lesson from this investigation was that all personnel undertaking safety-critical roles should adhere to the principles underlying the application of non-technical skills to ensure that they share the same mental models and have a clear understanding of what is required of themselves and others to complete the task safely.
-
On 21 September 2020, a freight train on the East Coast Main Trunk line entered a section of track that the rail protection officer believed was part of a protected work area and which was already occupied by a contractor operating a hi-rail vehicle (Rail inquiry RO-2020-104 Safe Working Irregularity, Hamilton – Eureka 21 September 2020, Transport Accident Investigation Commission, January 2022). A collision between the train and the hi-rail vehicle was only avoided because the hi-rail vehicle had voluntarily cleared the track about five minutes earlier. The Commission found in part that:
…the rail protection officer and the train controller had a different understanding of where the blocking was required. As a result, both parties had different mental models of the area that was being protected…
- This investigation identified that KiwiRail recorded 61 track occupancy irregularities between June 2019 and May 2021. Of these 61 incidents, 21 were attributable to miscommunication.
- The Commission recommended that KiwiRail carry out an analysis of how it could best incorporate engineering control measures into both its current and future operations to minimise the risks that human factors play in effective protection for track workers (Recommendation 009/21).
-
On 16 December 2021, KiwiRail replied:
KiwiRail agrees with the intent of this recommendation. Work is currently underway to renew the Train Control system which will give us the technology to move to a form of hand-held track worker interaction in the future. The strategy is to deliver a Business Case for this next year to be funded and delivered in the 2025 - 2027 funding period. We will have completed implementation of the new Train Control system by 2025.
- The Rail Accident Investigation Branch (RAIB) of the United Kingdom has investigated 58 accidents and incidents involving track worker safety since 2005. In 2023 RAIB published a ‘summary of learning’ (Summary of learning – track workers, Rail Accident Investigation Branch, March 2023) on the protection of track workers from moving trains. The main themes from the RAIB summary of learning relevant to this inquiry are:
- planning work
- the quality of leadership on site
- the supervision and monitoring of trackworkers
- the way that information is presented to track workers
- the willingness of staff to challenge unsafe practices.
- The Australian Transport Safety Bureau (ATSB) released a report in 201723 developed after ATSB researchers reviewed 12,146 occurrence records from all state and territory rail safety regulators for the period July 2009 to July 2014. Of these, approximately 15 per cent were found to be associated with work on track.
-
In 2017, prompted in part by Commission recommendations, KiwiRail began the process of implementing Non-Technical Skills training for its staff. KiwiRail’s integration plan24 stated in part:
KiwiRail previously conducted Crew Resource Management training for its employees to provide them with skills and confidence to be in a position to challenge instructions whenever they felt the instruction was not correct or required expanding. This was to ensure the employee clearly understood the task or the instructions they had been given. This training required refresher training every two years.
Over time we have reviewed the Crew Resource Management process and have decided that it did not meet our requirements. As previously mentioned we have researched other rail operators through RSSB in the UK and Australia and found that the Non-Technical Skills strategy being used was a better fit for our operations. This review process has led to the establishment of this project.
- This training project was fully implemented within KiwiRail by 2020.
Organisational information
- KiwiRail Holdings Limited (trading as KiwiRail) was the operator of the railway line and employer of the track workers and train controllers.
- Transdev Wellington Limited (Transdev) was the operator of the passenger train and employer of the train driver.
Analysis Tātaritanga
Introduction
- Having systems in place to protect track workers from rail traffic is a fundamental premise of rail operations worldwide. Those systems are only effective if established procedures are followed. On this occasion, the track workers were able to avoid being struck by the passenger train by running through a dark tunnel to reach the exit. A potentially fatal accident was avoided by seconds.
- This section analyses the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations.
Factors leading to the incident
Train control
- Train control diagrams (see Figure 7 and Appendix 1) have been in use by rail operators worldwide for many decades. Whilst modern electronic and digital diagram systems are available, most operators have retained the paper-based diagrams for their ease of use, ready availability to reference and simplicity of storage.

- Paper-based diagrams do have disadvantages. High-traffic areas can become clustered with information, making them difficult to decipher. Train controllers do not have the ability to ‘zoom in’ to a specific area as they might with a digital diagram.
- Paper-based diagrams are also not interactive, in that their effectiveness is reliant on the train controller recording accurate information and also interpreting any recorded information on the diagram correctly. There is no risk control other than the train controller’s ability to carry out these functions accurately.
- Train controllers undertake 10 weeks’ classroom training, followed by up to 16 weeks’ on-the-job training before becoming qualified to work alone. They are regularly assessed and audited on safety-critical activities including diagram recording performance. Newly certified train controllers are audited at least six times within their first nine months of certification. The TC on duty at the time of the incident was considered by KiwiRail to be very experienced.
- The train control diagram is based on a simple time/distance graph with metrages and stations annotated on both the lefthand and righthand side of the document (see Figure 7). The train controller uses the diagram to record the movements of rail traffic (trains, hi-rail vehicles, track machines), establish the boundaries of track occupation areas and record any other information such as weather conditions and faults pertinent to safe working. Train control diagrams are kept by the rail operator for 10 years in case they may be required for reference.
- During the day before the incident a slip alarm had been activated at the 2.44 km mark between Wellington and Wadestown. The night-shift train controller annotated this alarm activation in green highlighter on the diagram (see Figure 8) and ruled a line from midnight until 0330. When at 0330 confirmation was received that the alarm had been reset, the night-shift train controller further annotated the diagram by crossing out the green highlighted line with black pen and writing “Track Cleared for Normal Speed’’, to denote that the alarm condition was no longer present.

- The TC started their shift at 0530 and was made aware during handover of the annotations on the diagram and the previous alarm activation. At that time of the morning there was little other information on the diagram as trains had not yet started running on the JVL. The TC was effectively looking at a blank diagram, except for the alarm activation and reset annotations at the 2.44 km mark.
- Minutes after the TC started their shift, the first JVL train departed Wellington heading towards Johnsonville. At about 0538 the train driver called the TC by radio to inform them that the train had stopped due to a TST activation south of tunnel 5 (see Figure 9).

- While the TC could offer no explanation why they incorrectly annotated this on the diagram at the same location as the previously annotated slip alarm (at the 2.44 km mark, between Wellington and Wadestown rather than at the 3.567 km mark between tunnels 4 and 5), it was likely because the now obsolete green highlighted line was a point of visual reference that stood out on the otherwise almost blank diagram.
- In turn, it was likely the incorrect annotation led the TC to make a false association between the earlier slip alarm and the TST activation when they were in fact two separate events.
- The actual location of the TST activation was just over one kilometre north of where it was annotated by the TC on the diagram.
- The TC continued their shift in what was becoming an increasingly busy environment as passenger train services resumed their normal week-day commuter schedule after a week of minimal activity because of the track evaluation vehicle issues.
- The TC was controlling the JVL, rail traffic on the Wairarapa line between Masterton and Wellington, and passenger trains on the Melling line. There was also a non-timetabled driver-training train operating on the JVL, which added to the workload.
- The timetable software not having been uploaded that morning because of the short notice of the resumption of normal operations, meant the TC had to be extremely vigilant for trains approaching or leaving Petone station. An error in the order of any of these trains would lead to significant passenger service delays.
- With this level of activity, the TC’s focus was directed at the task of running trains and not at the TST activation, as at this stage it was a relatively low priority.
- When a second train encountered a TST activation at the same location as the first, the issue became more pressing as it could potentially cause major timetable disruptions. The TC recorded the second TST activation on the train control diagram at the same incorrect location as they had recorded the first TST activation.
- The TC contacted 155, who initiated a ‘priority one’ job and began their callout process to notify infrastructure staff to attend.
- Because of staff absences, nobody on the callout list responded to 155, and the job remained unattended. However, by this stage the small rockfall that was causing the TST activations had been pushed away from the track by the passage of rail traffic to the point that it was no longer connecting with the TST levers and had therefore ceased to be an issue.
- When TW1 eventually responded to the 155 callout, seven hours had passed since the initial TST activation.
- The TC stated in their interview that by the time they received the initial telephone call from TW1 at about 1240 requesting track time, they had forgotten about the TST activations as none had been reported since about 0600 that morning.
Track worker
Safety issue: Short staffing resulted in a track worker undertaking a task when they were not fully qualified to perform the role and were not familiar with the work area.
- On the morning of the incident, TW1 was already engaged in track-work activities with their infrastructure team in Wellington yard. TW1 was qualified to take out track protection but was not in a supervisory position.
- Because of staff resourcing issues, TW1 was the senior member of the team and assumed the responsibility of acting as the ‘person-in-charge’ of the work taking place in Wellington yard. The regular supervisor of the infrastructure team that TW1 belonged to had worked night shift the previous evening and was not available for work that morning.
- When TW1 received notification of the issue on the JVL, they acted as they thought necessary to address the problem, as they were of the belief that the continuity of mainline passenger train services should take priority over yard maintenance.
- TW1 and TW2 acquired a KiwiRail work truck and travelled towards Crofton Downs with little preparation and without preparing a cohesive plan for the work. No job plan or hazard analysis was completed. No equipment was taken other than a Mis 71 pad and shovels to clear the rockfall. All communication was conducted using TW1’s personal mobile phone as portable radios, although they were available, were not uplifted by the trackworkers.
- During their interview, TW1 advised Commission investigators that they had not worked on the JVL very often as their infrastructure team was mostly utilised for work in yards. However, TW1 was aware that any work on the JVL required protection from train control in the form of electronic blocking.
- TW1, while acting with good intentions to attend to the fault, was not qualified in a supervisory position to plan, prepare or lead others to carry out the required work.
Substance use
- While TW1 tested positive for THC immediately after the incident, the level of impairment was not determined. TW1 left KiwiRail employment soon after the incident, and therefore secondary testing that may have indicated the level of impairment was not undertaken.
- While no determination has been made that drug-induced impairment was a factor in this incident, the Commission regards the use of recreational drugs by safety-critical transport personnel to be a significant safety concern.
- In 2015, noting several other cases in which performance-impairing substances had been detected in people in transport safety-critical roles, the Commission added an item to its Watchlist (the Watchlist draws attention of regulators, operators, the Government and people involved in transport every day to transport-related concerns of high social, economic or environmental risk, and systemic transport safety risks. For reference see https://www.taic.org.nz/watchlist): The Commission was concerned about the lack of effective regulation against substance use by people performing transport safety-critical tasks in a transport environment. Judgement, decision-making and reaction time can all be affected by the use of drugs or alcohol. The use of performance-impairing substances by people carrying out safety-critical tasks in a transport environment is a significant risk.
- The Commission will continue to monitor the incidence of accidents featuring alcohol or drug impairment and seek a regulatory environment that supports zero tolerance of alcohol or drug impairment in safety-critical transport roles.
The incident – protection establishment
Safety issue: The use of incorrect procedures to establish protection and ineffective communication between the train controller and TW1 indicate that non-technical skills were not being adequately utilised during a safety-critical task.
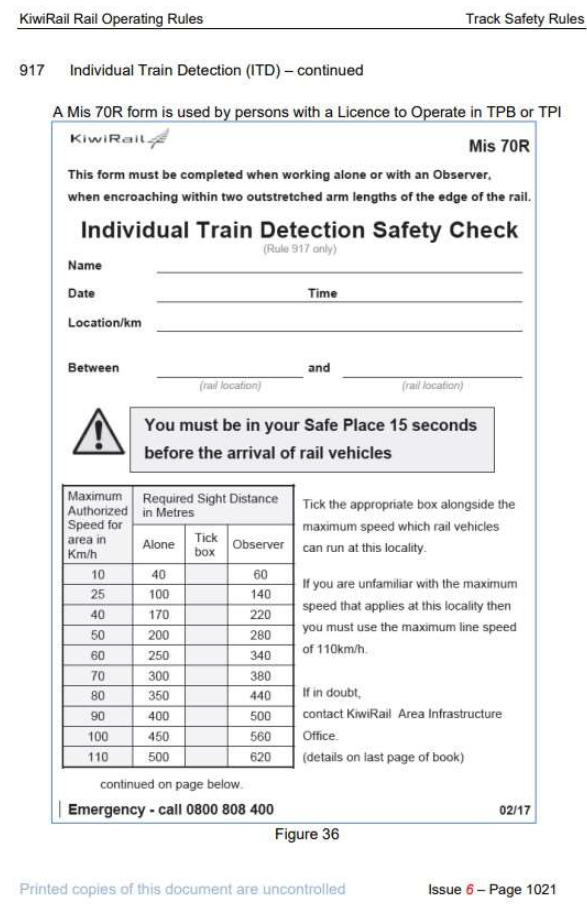
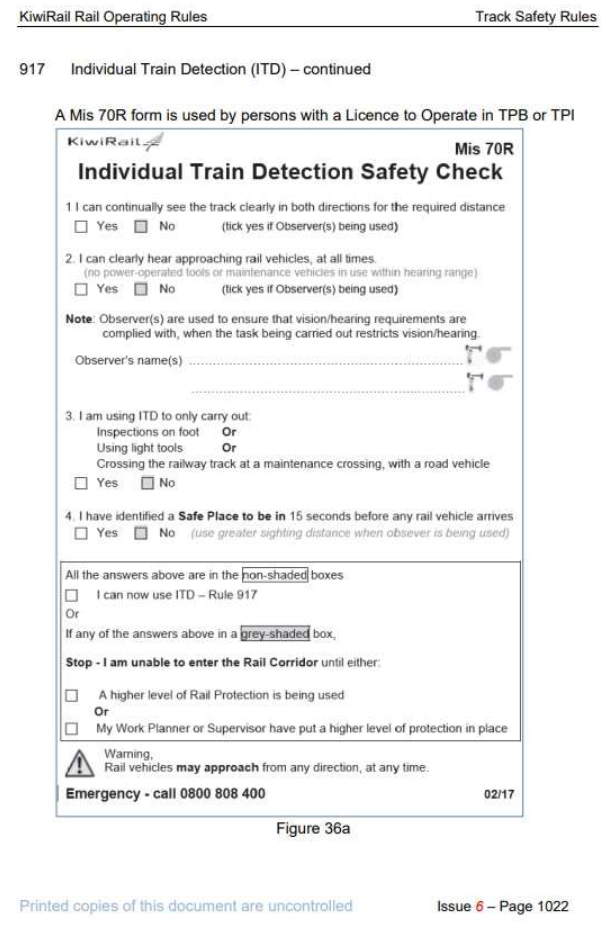
- When TW1 arrived at the 3.85 km mark and made initial contact with train control, a safe-working breach had already occurred, with the track workers making their way to the 3.85 km mark without protection in place. Protection in the form of blocking was required on the JVL for all trackside work. Protection in the form of individual train detection (ITD) (see Appendix 3) was not authorised for use on the JVL where, because of the geography of the terrain, the required clear sightline distances for ITD were not available. Blocking was required to walk alongside the track from Crofton Downs to the 3.85 km mark.
- The TC was unaware anyone was responding to the TST activation until unexpectedly receiving a telephone call from TW1 at the 3.85 km mark location seven hours after the TC had contacted 155.
- The TC, focused on train running, did not immediately recognise that TW1 should not have arrived at the calling location without any form of protection. They proceeded to issue the protection requested by TW1 to walk through the tunnel to the rockfall location.
- The TC advised TW1 that blocking was in place between 97 signal Wellington, and 4L signal Wadestown (see Figure 10). These locations for blocking were insufficient to protect the area the track workers were in. The TC very likely applied blocking to the incorrect area as they had formed an inaccurate mental model of the situation based on their earlier incorrect annotation of the TST activation location on the train control diagram.

- The incorrect diagram annotation likely led the TC to misinterpret the actual location of TW1, even though the location of “3.85 km, north of tunnel 5” was clearly stated by TW1.
-
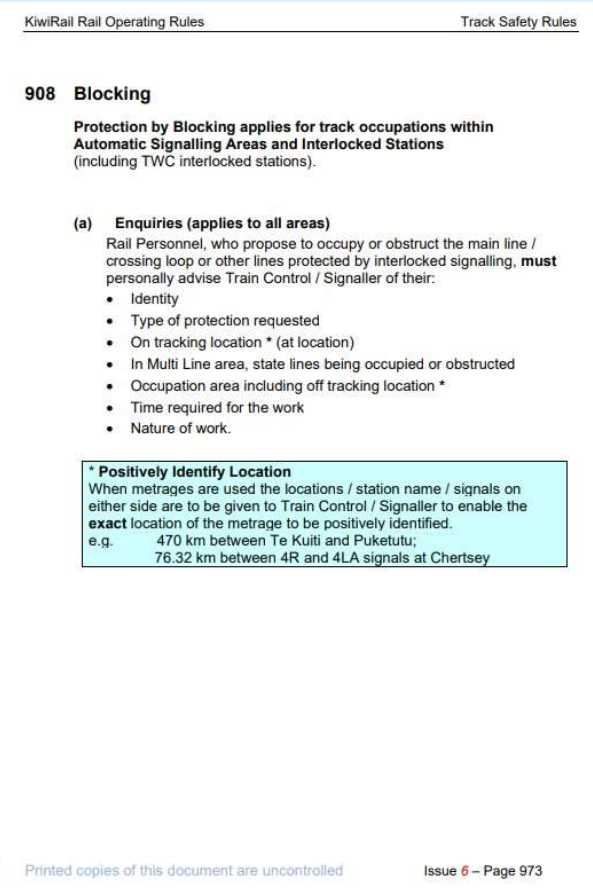
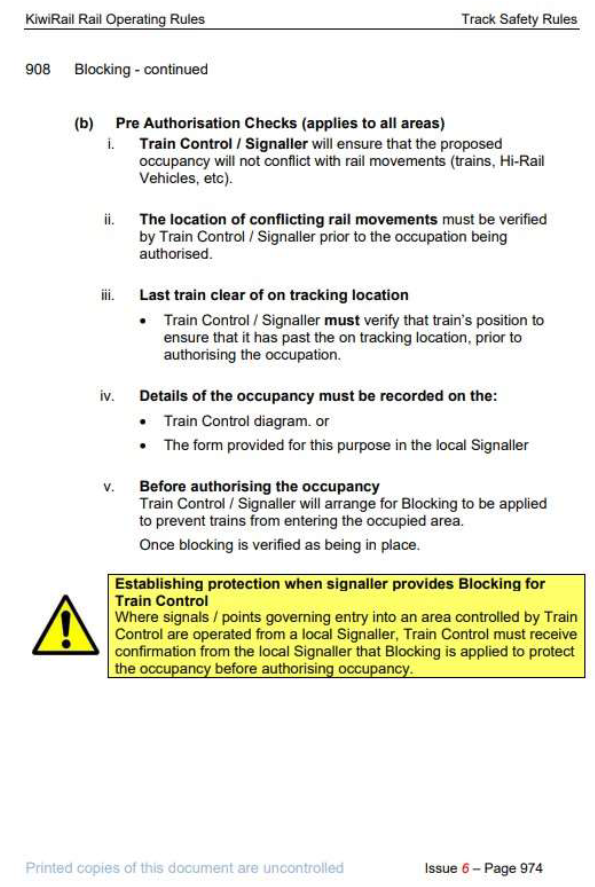
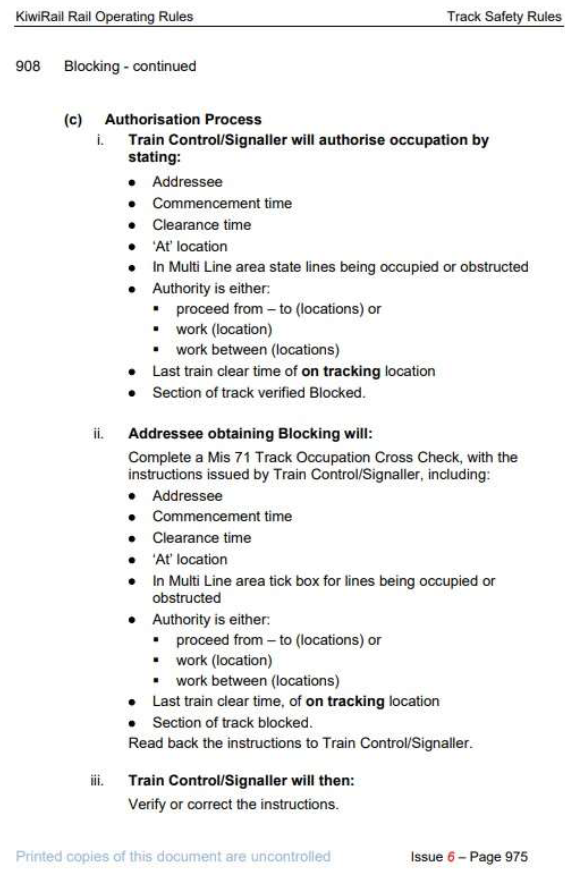
KiwiRail’s Rail Operating Rules and Procedures, Rule 908 – Blocking stated in part:
Rail Personnel, who propose to occupy or obstruct the main line/crossing loop or other lines protected by interlocked signalling, must personally advise Train Control/Signaller of their … On tracking location* (at location)
*Positively Identify Location
When metrages are used the locations/station name/signals on either side are to be given to Train Control/Signaller to enable the exact location of the metrage to be positively identified … [emphasis KiwiRail’s]
- The correct application of the above rule, by giving the station names on either side, would have required TW1 to inform the TC that they were at the 3.85 km mark, between Crofton Downs and Wadestown.
- Since the correct procedure was not carried out, an opportunity was missed for the TC to adjust their preconceived understanding of the track worker’s location, which the TC thought was between Wadestown and Wellington.
- Had this occurred, it would very likely have prompted the TC to verify TW1’s location by using both the train control diagram and the train control mimic screen to calculate where the correct blocking was required. Consequently, the TC would almost certainly have recognised that a train was about to enter the area for which blocking had been requested, and track time would not have been granted until the train was clear.
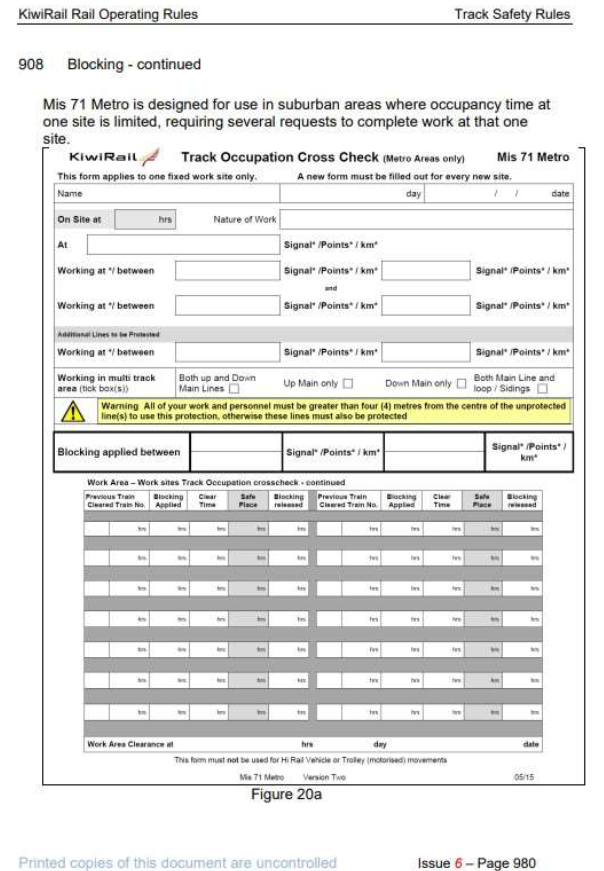
Mis 71 form
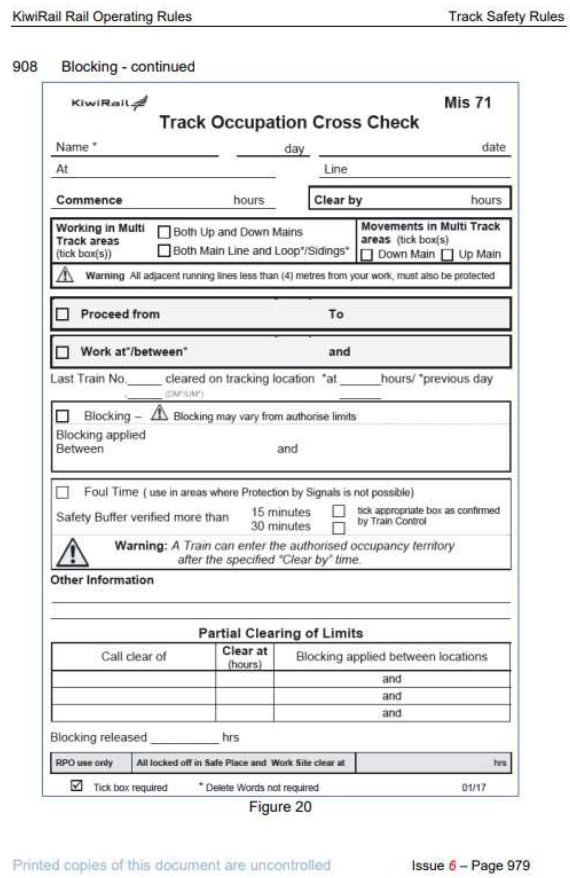
- Personnel requiring track time were required to complete a Track Occupation Cross Check form. This form was commonly referred to by KiwiRail personnel by its form number – Mis 71 (see Figure 11).

- Mis 71 forms were provided in A5 sized pads to be available to all staff that might be required to use them. Once completed the forms were to be kept as an auditable record.
- At the time of the incident, the Mis 71 form had a section to be filled out for the ‘At’ location (see Figure 12). This ‘At’ section did not include prompts to ensure the ‘At’ description complied with Rule 908 and identified the stations either side of the protection sought to enable the metrage to be confirmed.

- Had the Mis 71 form reflected the requirements of Rule 908 by including prompts for stations either side, TW1 would very likely have complied with exactly what was prompted on the form and their location would have been positively identified. Had this occurred the incident would almost certainly have been avoided.
Non-technical skills
- Non-technical skills can be defined as the cognitive, social and personal resource skills that complement technical skills and contribute to safe and effective task performance. Sub-categories of non-technical skills include situational awareness, communication, decision-making, leadership, teamwork, workload management and self-management.
- The effective use of non-technical skills is an important defence to capture and/or mitigate the effects of human error. This is even more important in systems that, in the absence of more robust engineering controls, are primarily reliant on individual performance and less-effective administrative controls. The TC and TW1 had both received training in non-technical skills. However, as this incident highlights, ineffective communication can render a system that is already over-reliant on administrative controls even more vulnerable to accidents and incidents.
- The likelihood of erroneous read-back and hear-back errors is increased when those communicating have a preconceived notion of what they are expecting to hear (expectation bias). While expectation bias cannot be eliminated, defences (such as specific phraseology and challenge-respond techniques) go some way to ensuring a complete and correct understanding is shared by both parties.
- On this occasion the TC misinterpreted the location described by TW1 as “3.85 km, north of tunnel 5” as being at the 2.44 km mark, which was the site of the previous slip alarm and where the TC had placed the TST activations earlier in the shift.
- While the TC had an incorrect mental model of the required blocking, it was incumbent on TW1 to be aware of what blocking was required, and to challenge what they were being told by the TC as being incorrect.
- Conversely, it was also incumbent on the TC to ensure that TW1 followed procedure by giving the station names either side of their call location.
- In this incident, all communication was conducted using telephones, as TW1 had not taken a portable radio to the site. Had radio communication been used, a more formal communication procedure should have been adhered to and this would have increased the likelihood of either party applying their non-technical skills training to challenge and/or correct the other. KiwiRail has taken action to restrict the use of telephones between train control and track workers (see para 5.5).
- Good communication is a key component of safety within the rail industry. In this incident the use of good communication skills would have helped to establish a shared mental model of the required blocking protection. Had the location of the blocking been challenged, a serious error very likely would have been identified and rectified.
Appendix 1. Train control diagram

Appendix 2. KiwiRail Rule 908–Blocking

Appendix 3. Rule 917 – Individual train detection