At 0707 on 10 January 2023, a hi-rail vehicle (HRV1) stopped on a curve near Te Puna so the Ganger could mark a worksite. A second hi-rail vehicle (HRV2), following two minutes behind, rounded the curve at about 38 km/h and struck the rear of HRV1 as TW1 was re-entering the cab. TW1 was thrown onto the ballast and injured, and equipment on HRV1 was damaged.
Executive summary Tuhinga whakarāpopoto



What happened
- At about 0707 (times used in this report are expressed in the 24-hour format based on New Zealand Daylight Time) on 10 January 2023, a Hi-Rail vehicle (HRV1) on-tracked at the Paparoa Road level crossing near Te Puna, approximately eight kilometres (km) west of Tauranga and near the 87-kilometre mark on the East Coast Main Trunk line (see Figure 3). It then began travelling northwest towards a planned worksite near Apata for an infrastructure team to carry out maintenance work.
- HRV1 was being driven by the infrastructure team’s supervisor (the Ganger) and there was one passenger, a track worker (TW1).
- A second Hi-Rail vehicle (HRV2), driven by another track worker (TW2), on-tracked at the same location two minutes after HRV1 and started travelling in the same direction towards Apata, following HRV1 to the worksite.
- The Ganger driving HRV1 stopped the truck in the middle of a left-hand curve, approximately 500 metres (m) from the on-tracking location, to mark a section of track that indicated the start of the worksite.
- Once stopped, the Ganger and TW1 both exited HRV1 and walked to the track in front of the vehicle. The Ganger then spray-painted markings onto the track while TW1 watched what the Ganger was doing.
- A short time later HRV2, driven by TW2, rounded the left-hand curve behind HRV1 travelling at approximately 38 kilometres per hour (km/h).
- When TW2 realised that HRV1 was stopped on the track, they attempted to stop by braking heavily. However, HRV2 collided with the rear of HRV1 while travelling at 38 km/h at the same time as TW1 was climbing back into the cab of HRV1.
- Upon impact TW1 was thrown off HRV1 onto the stone ballast at the side of the track. TW1 suffered bruising to their body and a lacerated finger. Metal cabinets on the rear deck of HRV1 were also shorn off their mountings and became unsecured.
Why it happened
- A radio call made by the Ganger to HRV2 stating that HRV1 was stopped on the track ahead was not received or acknowledged.
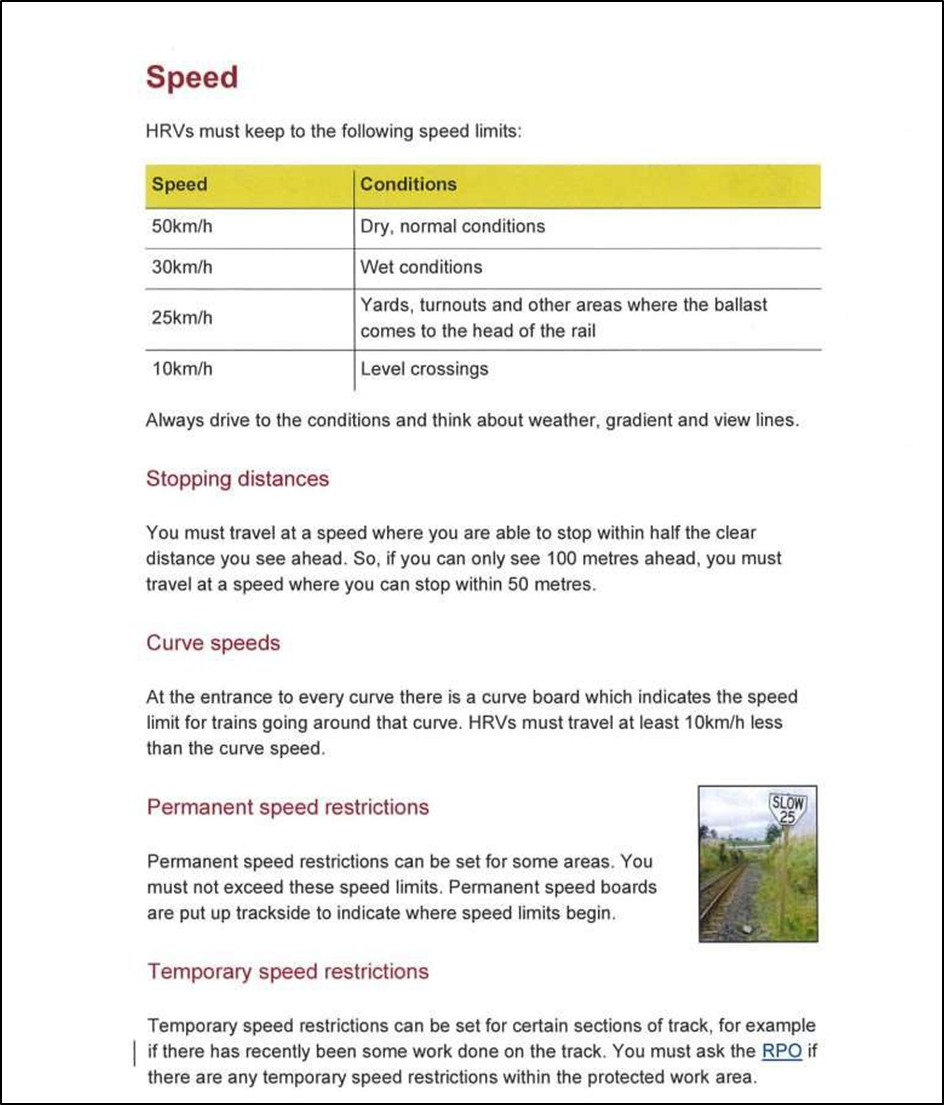
- HRV2 was travelling at a speed that did not reflect the conditions and was contrary to the requirements of KiwiRail’s Rail Operations Rules and Procedures.
- As well as carrying out the work task, the Ganger was conducting multiple roles including worksite supervisor, team trainer/instructor and rail protection officer. The Ganger was not adequately supported to carry out these roles while simultaneously supervising the safety of a relatively inexperienced team.
What we can learn
- Safety-critical tasks, such as operating HRVs on track, require a high level of focus, behaviour and communication.
- All rail staff should be aware of the possibility of conflicting rail traffic while working near vehicles stopped on track.
- Personnel involved with the loading of rail vehicles, including HRVs, should ensure the security of loads before travel to mitigate the consequences of a collision.
Who may benefit
- Rail operators, worksite supervisors, rail protection officers (RPOs), HRV operators, track maintenance personnel and people working around vehicles may all benefit from the findings in this report.
Factual information Pārongo pono
Narrative
Background
- The work gang operating on the day of the accident consisted of six people: the Ganger (worksite supervisor), who was also the RPO, and five track workers. The work gang was operating three Hi-Rail vehicles (HRVs): a heavy destress unit (HRV1), a tamper unit (HRV2) and a third unit (HRV3) (see Figure 4).

- The work gang was to travel from the on-tracking location to the worksite to conduct destressing operations.
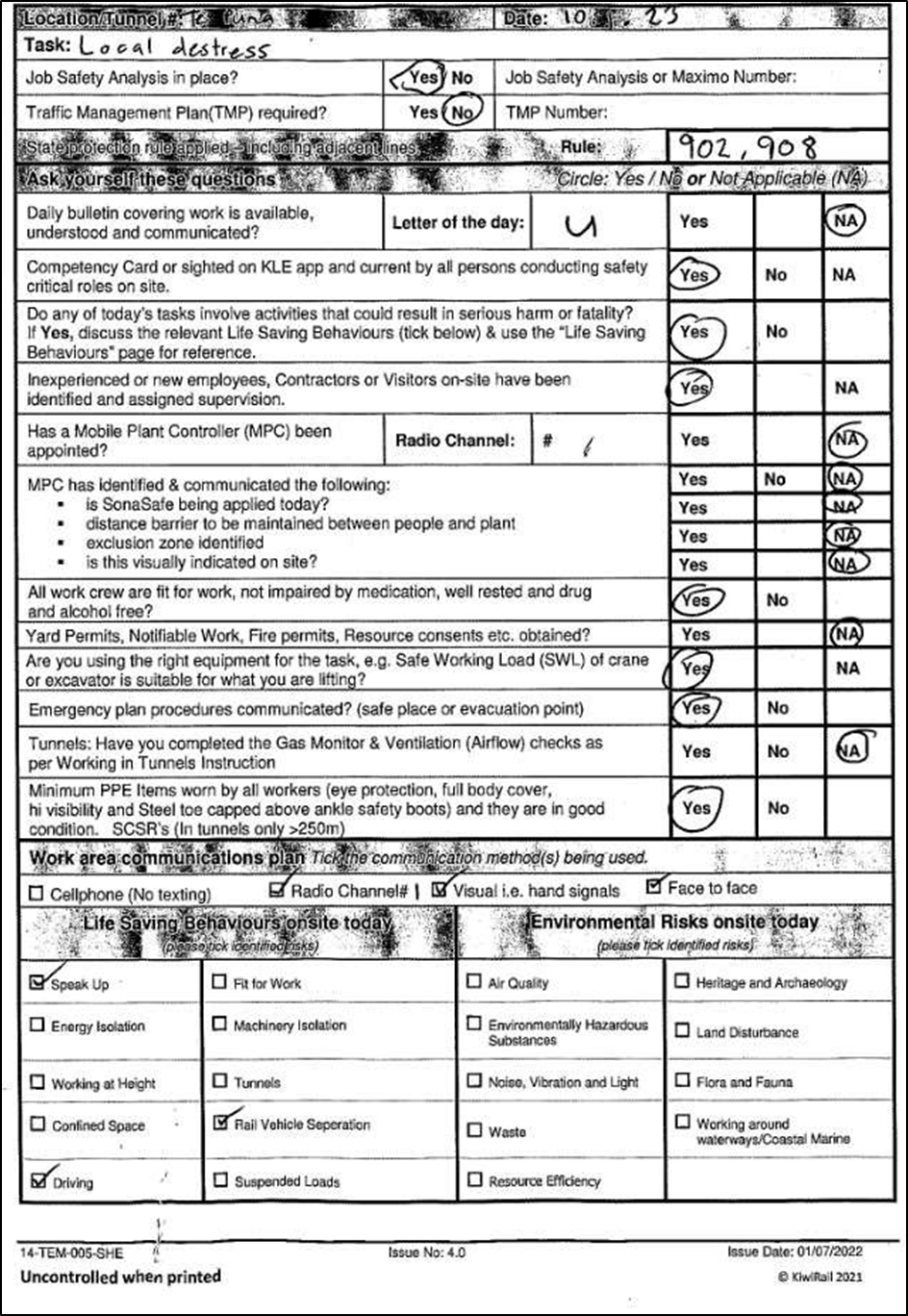
- On arrival at the on-tracking location, the work gang carried out a pre-start meeting. This included completion of a Job Plan using KiwiRail’s Job Plan Book (referred to as a TS90 book) and a safety-briefing on the work location, work tasks, protection arrangements, health and safety details, communications plan and specific site hazards (see Appendix 1).
- The specific site hazards for this day included rail vehicle separation, weather and driving/Hi-Railing. The safety-briefing did not include a diagram of the proposed worksite or how the activity was to be carried out, although there was a specific form in the TS90 book for this information that was not filled out.
- TW1 completed the Job Plan form and the Ganger conducted the safety-briefing. There was heavy rain on the morning of the accident and the safety-briefing was held in a group outside the vehicles.
The event
- At about 0707 on 10 January 2023, after receiving permission from train control and the necessary protections having been established, HRV1 on-tracked at the Paparoa Road level crossing, near the 87-kilometre mark on the East Coast Main Trunk line. It then began travelling towards a planned worksite near Apata.
- The Ganger was driving HRV1 and there was one passenger, TW1.
- The plan was for all three HRVs to on-track and travel to the worksite in the order of HRV1, HRV2 and HRV3. However, HRV3 did not have time to on-track before the accident occurred and it remained off track at the Paparoa Road crossing.
- HRV2 on-tracked two minutes behind HRV1, with a driver (TW2) and one passenger and began travelling in the same direction as HRV1 towards the planned worksite (see Figure 5).

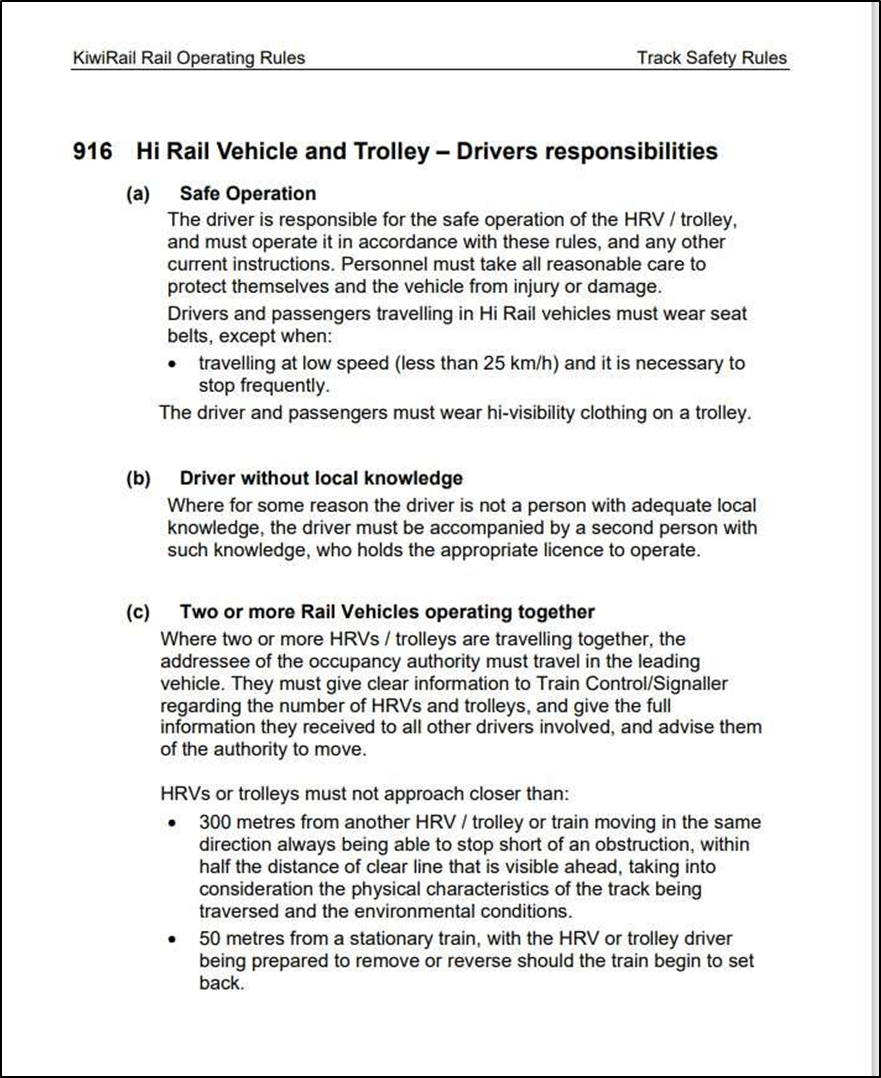
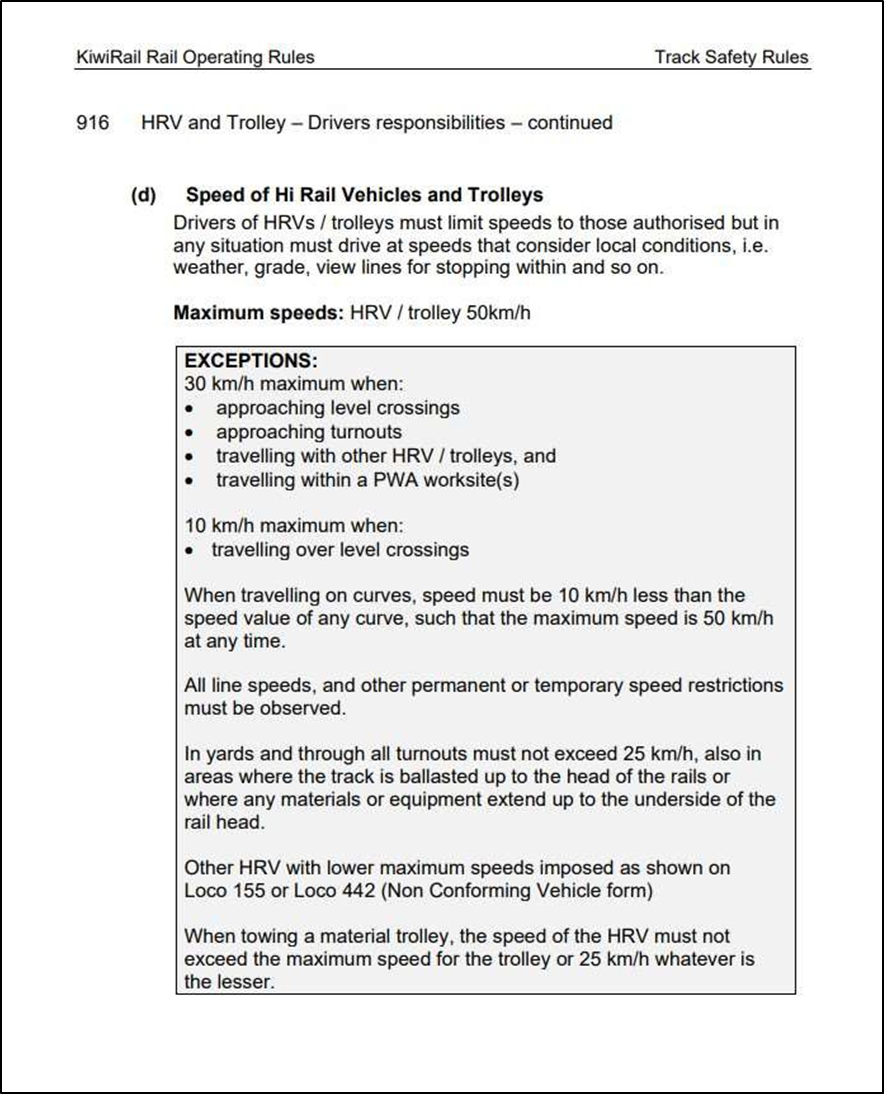
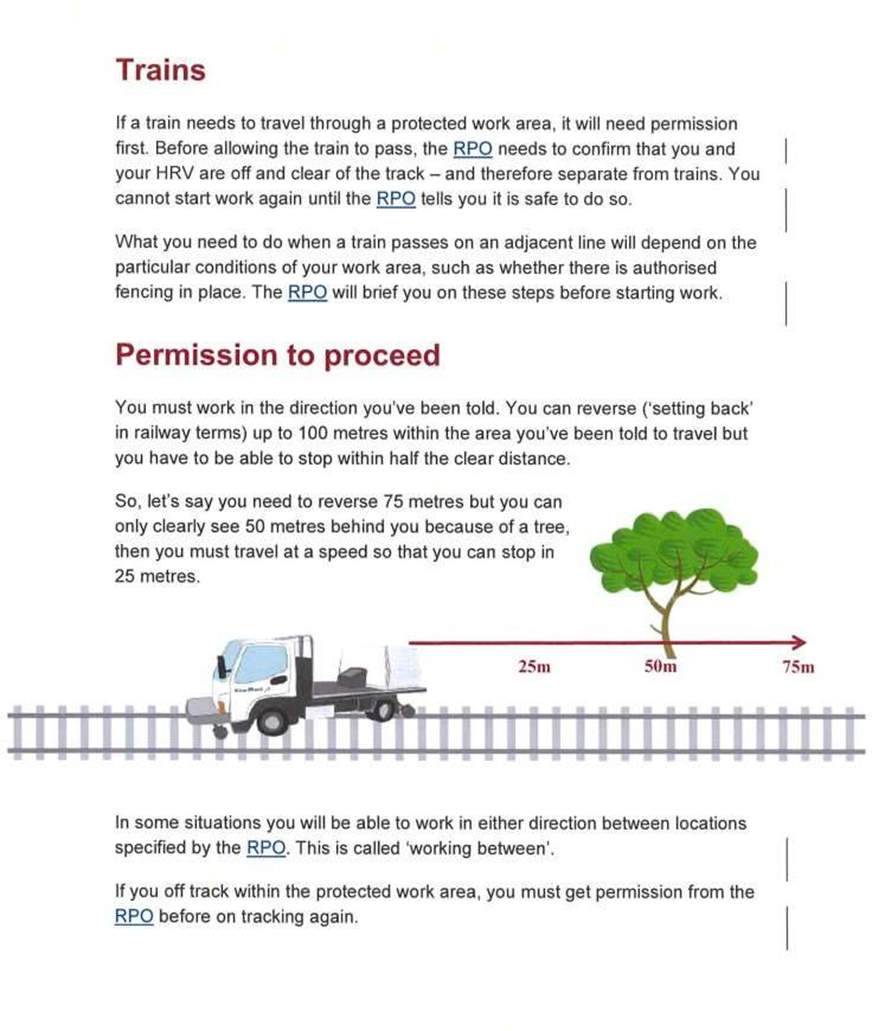
- Because of the wet weather conditions at the time and of also travelling in convoy, the HRVs should have been travelling at no more than 30 kilometres per hour (km/h), and at such a speed that they would have been able to stop within half the clear distance that could be seen ahead (KiwiRail Rail Operating Rules – Track Safety Rule 916(c)-(d) – HRV and Trolley – Driver’s responsibilities (also see Appendix 3)).
- At about 0711 the Ganger stopped HRV1 to mark a section of the track with spray paint. The Ganger and TW1 left the cab of HRV1 and were standing on the ballast in front of the vehicle.
- The Ganger stated that on stopping they made a call on the radio to inform HRV2 that HRV1 had stopped. No response or acknowledgement was received for this radio call from HRV2 and the occupants of HRV2 both stated that they did not hear a call on the radio.
- At 0712 TW2, the driver of HRV2, which was travelling at approximately 38 km/h, was not aware that HRV1 had stopped. On seeing the vehicle after rounding a bend and realising that HRV1 was not moving, TW2 attempted to stop HRV2 but was unable to do so before it collided with the rear of HRV1 (see Figures 6 and 7).


- The Ganger stated that on sighting the incoming vehicle, and realising HRV2 would not be able to stop in time, they shouted a warning to TW1. However, TW1 had neither seen the approaching HRV2 nor heard the warning and was in the process of climbing back into the cab when the collision happened.
- As a result of the collision HRV1 was shunted 13 metres (m) forward from its stationary position. Global Positioning System (GPS) data shows HRV1 accelerating from 0 km/h to 10.2 km/h one second after the collision, then moving at 15.9 km/h two seconds after the collision, 12.7 km/h three seconds after the collision, 9.5 km/h four seconds after the collision and 3.2 km/h five seconds after the collision before coming to a stop six seconds after the collision.
- TW1 was in the process of climbing from the trackside into the cab when the collision occurred and as a result was thrown from the vehicle onto the ballast, suffering bruising and a lacerated finger requiring stitches.
- Immediately after the collision the Ganger went to the assistance of TW1. On assessing that TW1 required medical treatment the Ganger also checked the occupants of HRV2 before instructing the work gang to reverse the HRVs to the original on-tracking location to clear the track. TW2 and their passenger reversed to the off-tracking location in HRV2, followed by the Ganger driving HRV1 with TW1 as passenger.
- At 0813, one hour after the accident, the Ganger advised train control that an accident had occurred, and that all vehicles and personnel were now clear of the track.
- On being advised that an accident had occurred train control escalated the situation to the Network Control Manager13 and an investigation was initiated by KiwiRail.
- TW1 was taken to hospital in HRV3 for medical attention. The HRVs and the work gang returned to Tauranga depot where the Ganger and TW2, as drivers of the HRVs, underwent drug and alcohol testing.
Personnel information
- The Ganger had been employed by KiwiRail since August 2016. On 28 September 2020 they completed the Ganger’s Skills course (KiwiRail’s leadership course for worksite supervisors). Post-accident drug and alcohol testing was conducted and indicated a negative (passed) result.
- TW2 had been employed by KiwiRail as a track worker since October 2021. On 14 June 2022 they completed the Track Protection Basic Machines course (full and final certification to operate a Hi-Rail vehicle within a protected work area). Post-accident drug and alcohol testing was conducted and indicated a negative (passed) result.
Vehicle information
- Both HRVs were Mitsubishi Fuso Canter trucks that had been fitted with retractable rail wheel equipment allowing them to travel on both road and rail. Both trucks held current certificates of fitness and had been recently serviced.
Meteorological information
- Between 1 January 2023 and 11 January 2023, 119 millimetres (mm) of rain was recorded in Tauranga as a result of ex-tropical cyclone Hale, compared to 22.2 mm for the same period the year before. Although there was heavy rainfall in the area on the morning of the accident, visibility was not affected. However, compared to dry conditions, the wet rails would have reduced the braking efficiency of the HRVs.
Recorded data
- The Commission obtained recordings of radio communications between the Ganger and train control. Radio communications between HRVs are not recorded.
Other data sources
- HRV1 and HRV2 were both fitted with ‘Navman’ GPS equipment. The Commission obtained data from the GPS equipment for use in its investigation.
Site and wreckage information
- HRV1 received superficial damage to the rear of the vehicle.
- HRV2 received substantial damage to the front of the vehicle and to the retractable Hi-Rail equipment.
- The Commission issued a Protection Order on both vehicles to conduct testing and evidence gathering.
Medical and pathological information
- TW1 was treated for bruising and required stitches to a lacerated finger.
Tests and research
- During interview, TW2 stated that they thought HRV2 had ‘lost power’ when they applied the brakes on seeing HRV1. The Commission engaged a Mitsubishi agent to conduct fault data analysis testing on HRV2. The fault data analysis found no evidence of power loss leading up to the accident. GPS data indicated HRV2 was travelling at an almost steady speed without significant deceleration until the time of impact (see Figure 8).

- Commission investigators also conducted a re-enactment of the accident using two HRVs of the same type as those involved in the collision and in similar weather conditions to determine sighting and braking distances.
Previous occurrences
- On 24 April 2020, a Mitsubishi Fuso Canter HRV was struck by a freight train at Limeworks Road level crossing between Milton and Henley (TAIC report RO-2020-102 https://www.taic.org.nz/inquiry/ro-2020-102). The investigation found that the accident occurred in track warrant territory as a result of the HRV driver on-tracking before a train travelling towards their location had cleared, contrary to the track warrant requirements.
- On 2 May 1996, two HRVs collided near Kotemaori (TAIC report RO-1996-104 https://www.taic.org.nz/inquiry/ro-1996-104). The two vehicles were working in the same area independent of each other when one vehicle rounded a bend and encountered the other vehicle ahead of it travelling in the same direction but at a much lower speed. The investigation found that “the cause of the collision was insufficient information available to the employee in charge of one of the Hi-Rail vehicles.”
Organisational information
- KiwiRail Holdings Limited (trading as KiwiRail) was the operator of the railway, owner of the HRVs and employer of all the workers involved.
Analysis Tātaritanga
Introduction
- The safety of multiple vehicles working together within a protected work area relies on all operators following established rules and procedures to maintain safe vehicle separation.
- The following section analyses the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations.
Training
Safety issue 1: Training of staff covered operating a HRV within a protected work area but assumed it occurred under direct supervision of a rail protection officer or qualified safety protector. The training did not adequately address independently travelling longer distances to get to the work area. Had the track workers understood the risks involved with travelling, the accident would likely not have occurred.
- TW2 (the driver of HRV2) completed a two-day Track Protection Basic – Machines (TPBM) course and received full and final certification to operate a HRV within a protected work area on 14 June 2022 – six months before the accident.
- The TPBM workbook contained information for operators of HRVs that aligned with KiwiRail’s Rail Operating Rule 916 – Hi Rail Vehicle and Trolley – Drivers responsibilities (see Appendices 2 and 3)
- Content of the TPBM course included:
- Introduction to TPBM
- Protected Work Areas
- Radio communication
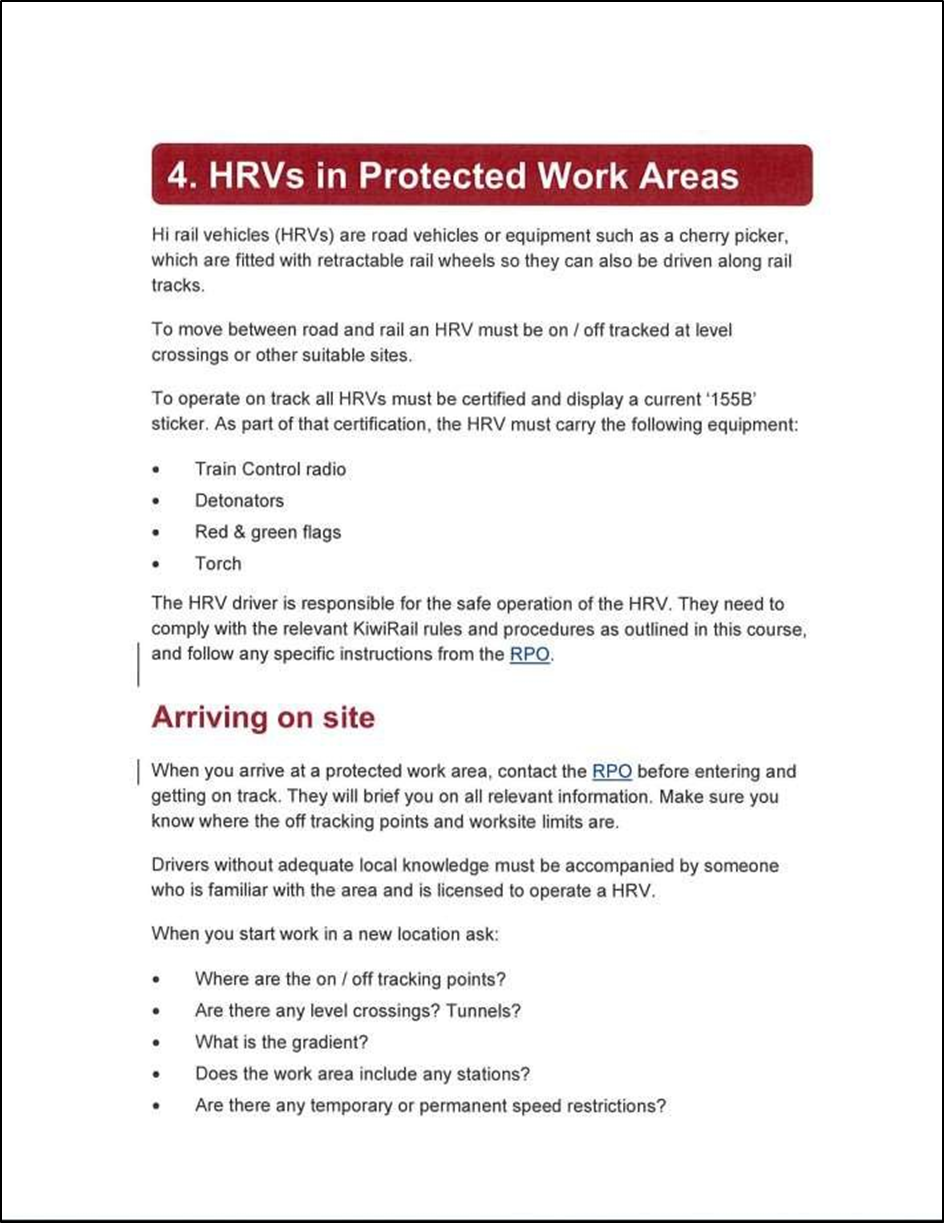
- HRVs in Protected Work Areas
- Emergency situations
- Operating a HRV
- Theory assessment
- On job training assessment
-
Rather than being a comprehensive HRV training programme, the TPBM course was designed to give personnel operating HRVs (such as Hi-Rail diggers and other maintenance vehicles) a basic understanding of the requirements of arriving on site, on-tracking and working on-track in a protected work area under the supervision of a RPO. This basic course was considered necessary as some operators, such as non-KiwiRail contractors, may not have been familiar with KiwiRail’s HRV safety requirements. The TPBM workbook stated in part:
Once you have completed the theory course and on job training, you will have KiwiRail’s Licence to Operate: TPBM. This means you will be able to safely use a hi rail vehicle in a protected work area – where a qualified safety protector is present at all times. [Emphasis KiwiRail’s]
- TW2 did not drive a HRV on a daily basis, as this task was shared between those members of the work gang with the necessary qualification. At the time of the accident, TW2 had been TPBM certified for six months and had not received any safety observations to confirm competency during that time.
- TW2 stated that they had not worked at the Apata worksite before and were not “100 per cent sure where they were going” but had simply intended following the lead HRV.
- When HRV1 on-tracked and began travelling to the worksite in front of HRV2, TW2 was left unsupervised, as the passenger in HRV2 was not TPBM qualified and was also unfamiliar with the area.
-
This was contrary to instructions given in the TPBM workbook, and also KiwiRail Rule 916(b) which stated:
Driver without local knowledge
Where for some reason the driver is not a person with adequate local knowledge, the driver must be accompanied by a second person with such knowledge, who holds the appropriate licence to operate.
- The effects of the lack of direct supervision may have been mitigated if the Ganger had remained in constant radio communication with TW2 to monitor their progress during the trip from Paparoa Road to the work site. However, this communication did not occur. No pre-start radio checks had been conducted that morning to ensure the HRV radios were working correctly. TW2 stated they did not check the state of the radio when they entered HRV2; they recalled that it was turned on but were unaware if the volume was up or if it was on the correct working channel.
-
The radio call the Ganger stated they made to the following HRVs to advise that HRV1 was stopped, was not received by TW2 and there was no acknowledgement of the message. The TPBM workbook stated in part:
Acknowledgements
All radio messages must be acknowledged. The person sending the message must not assume it has been received until it is acknowledged.
And further stated in part regarding radio testing:
Testing the radio
To be confident that people can hear and understand your message, you need to know that your radio is working properly and if you can communicate with another radio.
You need to check the channel is clear and carry out a call to test how well you can be heard.
- Had the procedures been followed to test that the radios were working correctly, and the message that HRV1 was stopped been acknowledged, the accident would likely not have occurred.
-
The Ganger, also acting as RPO, was required to travel in the lead vehicle of the convoy to comply with KiwiRail Rule 916(c), which stated in part:
Where two or more HiRail vehicles/trolleys are travelling together the addressee of the occupancy authority must travel in the leading vehicle…
And also to comply with the TPBM workbook, which stated in part:
If HRVs are travelling in a convoy then the RPO will be in the leading vehicle. They will inform all other drivers about information they receive from train control and will provide permission to travel.
- The requirement for the Ganger to travel in the lead vehicle effectively left TW2, who had minimal training and was unsupervised, on their own to drive the HRV through an area they were not familiar with, and with only a basic understanding of the worksite location.
- When HRV2 rounded the bend at over 38 km/h and TW2 saw HRV1 ahead, it took TW2 a moment to realise that HRV1 was stopped on the track and that immediate action needed to be taken.
- Upon realising HRV1 was not moving, TW2 estimated they were about 12 m from the vehicle when they started braking. This estimation is broadly supported by the GPS speed data obtained by the Commission.
- To comply with KiwiRail’s Rule 916(d) and the guidelines stated in the TPBM workbook, TW2 should have been travelling at no more than 30 km/h and at such a speed that they were able to stop in half the clear distance ahead.
- It was very likely that as a result of a combination of the above conditions, the application of HRV2’s brakes occurred too late to avoid a collision with HRV1.
- No action has been taken to address these safety issues. Therefore the Commission has made a recommendation in Section 6.
Safety issue 2: KiwiRail had not identified HRV cabs as being a safety-critical area so there was no enhanced training on the need for a high level of focus, behaviour and communication. Had track workers received such enhanced training, the accident would likely not have occurred.
-
There was scant information in the TPBM workbook about safe working within the cab of a HRV. However, it did state in part:
The HRV driver is responsible for the safe operation of the HRV. They need to comply with the relevant KiwiRail rules and procedures as outlined in this course, and follow any specific instructions from the RPO.
- The RPO on this occasion was also the Ganger, travelling in a separate vehicle, who had not issued any specific instructions to TW2 other than the unacknowledged radio call that HRV1 had stopped.
- During their interview, TW2 stated they had not been advised that a HRV cab was a safety-critical area18, and therefore they had not considered that it was.
- TW2 also stated that just before the accident they had been engaged in conversation with the passenger and they were not fully focused on the track ahead.
- Nevertheless, a track worker in charge of a HRV not being aware through training of the safety-critical nature of the task and of the need for a greater level of attention is of concern to the Commission.
- No action has been taken to address these safety issues. Therefore the Commission has made a recommendation in Section 6.
Support for the Ganger
Safety issue 3: The Ganger did not have adequate support to conduct multiple roles, including worksite supervisor, team trainer/instructor and rail protection officer, as well as carrying out the work task. Had the Ganger been able to delegate some of the workload it is likely the safety-critical tasks would have been more effectively supervised and the accident would likely not have occurred.
- The Ganger was first employed by KiwiRail as a track worker in 2016. In 2020, they completed the ‘Ganger’s skills’ course, a leadership-focused course provided by KiwiRail with the stated intention to “create a pathway for future leaders to successfully lead teams”.
- This course should have been followed by further training on business management and leadership. However, this further training was postponed because of the COVID-19 pandemic and had not restarted before the accident.
- The Ganger was assigned the members of the work gang as each of them completed initial KiwiRail induction training. Of the five members of the work gang, only one track worker in HRV3 had more than 18 months’ experience, and they were still at the on-tracking location when the accident occurred.
- In addition to carrying out any assigned work tasks, the Ganger bore the responsibility for the instruction of new staff in all aspects of track work, including health and safety.
- The Ganger also acted as the RPO at worksites, communicating with train control to establish protection for all personnel within the protected work area and ensuring those personnel were adhering to safety requirements.
- The responsibilities that came with being a Ganger and a RPO were substantial and would have been mitigated by the availability of adequately experienced staff to oversee less experienced staff during routine tasks.
- While the Ganger tried to allow less experienced staff to conduct tasks, such as recording the day’s safety plan, the Ganger was then responsible for checking that all of these tasks had been completed correctly.
- During their interview the Ganger stated that they faced a considerable amount of pressure to complete the work gang’s planned work to the required standard while simultaneously training the work gang to do that work.
-
During the investigation the Commission asked KiwiRail to provide its policies on the acceptable ratio of trainees/inexperienced staff assigned to a single direct supervisor. On 12 June 2023 KiwiRail replied:
There is no policy that states the acceptable ratio of trainees/inexperienced staff vs a supervisor. We very rarely get in the position where we have more than 1 trainee at one time with 1 gang so can manage internally.
We do have a buddy system that is part of the new employee induction process where an experienced employee is assigned as a Buddy to a new employee, this doesn’t necessarily need to be the Ganger/Supervisor, but someone to ensure the Safety of the new employee and to answer any queries [sic].
- However, this was not the situation the Ganger was operating in at the time of the accident; they were the only experienced person on site and acting as ‘Buddy’ to every other person on site out of necessity. KiwiRail’s ‘Buddy’ system was ad hoc and was not in place for the work group at the time of the accident. There remains a gap in KiwiRail’s policies for when there is more than one trainee at one time with one gang.
- Had there been more experienced staff available to assist the less experienced staff, adequate supervision of safety-critical tasks, such as operating HRVs, would likely have occurred and the accident would likely not have happened.
- No action has been taken to address this safety issue. Therefore the Commission has made a recommendation in Section 6.
Non-contributory factors
Post-incident procedures
- Immediately following the accident, the Ganger’s primary concern was for the wellbeing of their staff. The Ganger assessed if anyone was injured and provided first aid to TW1.
- The Ganger made the decision to reverse both HRVs back to the Paparoa Road crossing, off-track and transport TW1 to hospital.
- The Ganger contacted the driver of HRV3 and instructed them to remain off-track while HRV2 and HRV1 reversed towards the crossing.
- On arrival at the crossing, both HRV2 and HRV1 off-tracked. TW1 transferred to HRV3 and was taken to hospital for assessment.
- Once the situation had stabilised, the Ganger attempted to contact their line manager for direction and advice, but their phone was turned off as they were on leave. The Ganger then called the Production Manager but was again unsuccessful. The Ganger then called the Regional Manager and also received no answer. Eventually the Ganger was able to contact the Production Manager who enquired about the wellbeing of the work gang, asked the Ganger if they had marked up the site and advised the Ganger that they would start the investigation process.
- During their interview the Ganger could not recall being trained to freeze an accident site and was unable to describe the process or where to find the procedure.
- The procedure for what actions to take following an incident are provided in the back pages of KiwiRail’s ‘TS90’ book – the Job Plan book that the Ganger had briefed the work gang from about 10 minutes before the accident (see Figure 9).

- The Ganger was under pressure during the aftermath of the incident and was acting as they felt necessary to seek urgent medical treatment for TW1. However, one of the first actions they should have taken was to contact train control and advise of the situation.
- Advising train control would have afforded the Ganger the opportunity to deal with the situation at hand while train control made the necessary arrangements for medical attendance, halting rail traffic in the area, directing assistance to the scene and a multitude of other actions that could have assisted the Ganger who was working in isolation.
- The Ganger did not advise train control that there had been an accident until just over one hour after the collision, when at 0813 the Ganger notified train control that all personnel and machinery were clear, and the protection established for the work area could be rescinded. When train control acknowledged this the Ganger informed them that there had been an ‘incident’ and they would not be requiring further track time that day.
- It was on receipt of this information that train control informed the Network Control Manager, who began making enquiries into what had occurred and initiated the investigation process.
- By not immediately informing train control of the accident, an opportunity was lost for support to be provided earlier to the Ganger and for the scene to be frozen to preserve evidence that could have been crucial to an investigation had the circumstances been more serious.
Working near vehicles on track
- Moments before the accident, the Ganger and TW1 were standing directly in front of HRV1 while the Ganger marked the track with spray paint.
- KiwiRail rules are silent on working around vehicles on track while there is following traffic in the area.
- Had the Ganger and TW1 still been in front of HRV1 when it was struck from the rear by HRV2 they would have likely sustained serious injuries based on the rate HRV1 accelerated on impact.
- Although not contributory to this accident there is a key lesson that all rail staff should be aware of the possibility of conflicting rail traffic while working near vehicles stopped on track.
Crashworthiness
- The Commission found that on impact the four 8mm steel bolts that secured two metal cabinets containing heavy equipment were shorn from their mountings on the deck of HRV1.
- The Commission also found that tanks containing flammable welding gas were not secured sufficiently on the deck of HRV1 and were attached to the metal cabinets that became unsecured when the bolts were shorn off during the collision (see Figure 10).

-
This collision between the two HRVs occurred at a relatively low speed, and with little resistance when HRV1 began moving on impact.
-
The Commission is concerned that had one of the HRVs, which can travel on both rail and road, been involved in a rail incident at a higher impact speed the consequences of the load being unsecured could have been serious.
-
Although the unsecured load was not contributory to this accident, there is a key lesson for personnel involved with the loading of rail vehicles, including HRVs, that they should ensure the security of loads before travel to mitigate the consequences of a collision.
Appendix 1. Job Plan for 10 January 2023

Appendix 2. Excerpts from TPBM workbook
Appendix 3. KiwiRail Rail Operating Rule 916 Hi Rail Vehicle and Trolley – Drivers responsibilities