Safety issues for Airwork Flight Ops: fuel checklists, crew training, control centre comms, weather info, crew compliance with manuals, safety management system. No new recommendation because all issues addressed. A Boeing 737 freighter landed with fuel exhaustion imminent because centre fuel tank pumps were switched off for whole flight.
Executive summary Tuhinga whakarāpopoto


What happened
- On 7 June 2022, Boeing 737 registration ZK-TLL, operated by Airwork Flight Operations Limited (the operator) as flight number AWK2, landed at Auckland Airport after a night flight from Sydney. It had been a dedicated freight flight with two crew on board.
- After landing and while taxiing the plane to stand, the flight crew noticed that the centre fuel tank still had 4000 kilograms (kg) of fuel, but there was minimal fuel left in the two main tanks that were feeding the engines. They discovered that the centre fuel pumps had remained off for the entire flight when they should have been selected on during the engine start procedure in Sydney.
Why it happened
- The Transport Accident Investigation Commission (Commission) found that the flight crew omitted to turn on the centre fuel pumps when preparing the aircraft for the flight.
- The distractions of a last-minute change to the departure runway and an impending airport curfew very likely contributed to the omission.
- The Commission found that the flight had departed Sydney with a flight plan that nominated alternate aerodromes that were not compliant with regulatory or company flight-planning requirements. The operator’s operational staff had not provided weather updates and flight planning for the flight as prescribed in their manuals.
What we can learn
- Pilots need to ensure that procedures and checklists involving critical aircraft systems are completed with rigour and be aware of potential distractions.
- Operational staff need to follow the procedures detailed in their manuals to provide support to flight crew for extended-range flights.
- Pilots should ensure that flight plans for their flights are compliant with operator and regulatory procedures for alternate aerodrome planning.
Who may benefit
- Pilots, operators and operations staff will benefit from reading this report.
Factual information Pārongo pono
Narrative
- On the evening of 6 June 2022, the operator of Boeing 737 (B737), registration ZK-TLL, conducted a scheduled two-sector night freight flight from Auckland to Sydney and Sydney to Auckland. The first sector, Auckland to Sydney, had a callsign (flight number) of AWK1 and the return sector, Sydney to Auckland, had a callsign of AWK2.
- The return Sydney to Auckland flight landed at 0340 (all times in this report are in New Zealand Standard Time (NZST), which is Coordinated Universal Time (UTC) – the primary time standard used globally to regulate clocks and time +12 hours, and are in the 24-hour format) on 7 June 2022. After landing the flight crew noticed that there was substantial fuel remaining in the center (Boeing (the manufacturer) documentation spells center in this manner, and for consistency it has been used throughout this report when referring to fuel tanks and fuel pumps) tank, with minimal fuel in the main tanks, and that the center fuel pumps were switched off.
Background
- The flight crew consisted of a training captain and first officer. The first officer was new to the company and was undertaking planned support line training on these two sectors following a recent unsuccessful check to line flight.
- The operator’s Operations Control Centre (OCC) (A description of the OCC and its functions can be found in paragraph 2.38 of this report) dispatcher generated a weather briefing at 1720 and flight plans for both sectors at 1747. The flight plan for the return sector Sydney to Auckland nominated Palmerston North as the alternate aerodrome (alternate) for Auckland, and Sydney and Auckland were listed as the two Extended Diversion Time Operation (EDTO) (‘Extended Diversion Time Operation’ is explained in paragraph 2.35) alternates. This was based on aviation weather forecasts issued by the Meteorological Service of New Zealand Limited (MetService)(See paragraph 2.26 for a description of the MetService) at 1709 for Auckland and 1112 for Palmerston North.
- The flight crew reported to the operator’s Auckland base at 1845 and conducted preflight weather briefings and flight planning for both sectors. Flight AWK1 departed six minutes before scheduled at 1954 and was airborne at 2008. The sector to Sydney was uneventful, but the flight arrived 34 minutes late at 0004 on 7 June due to strong headwinds across the Tasman Sea.
Sydney to Auckland sector
- Sydney airport has a government-mandated curfew commencing at 0100.
- On arrival at Sydney the flight crew were advised by an email from the OCC that fog was forecast at Auckland for the return sector, but they were not provided with updated forecasts for Auckland or any alternates. The flight crew responded to the email by requesting that an extra 1000 kg of fuel be loaded for the return sector.
- When the flight crew was ready to depart Sydney as flight AWK2, they requested pushback. They were informed by air traffic control (ATC) that due to noise-abatement procedures they would have to depart from runway 16R rather than the planned runway 16L, runway 16R being less noise sensitive. Pushback was delayed while the flight crew made the necessary changes to the flight management computer and re-briefed the departure.
- When these tasks were complete, the flight crew recommenced preparation for pushback. It was at this stage that the center fuel pumps should have been turned on as part of the operator’s Boeing 737-300/-400 Flight Crew Operations Manual (FCOM) Before start procedure.
- The flight was pushed back at 0051 and airborne at 0102. The return sector was relatively short due to strong tailwinds, with a flight time of two hours, 38 minutes against a scheduled time of three hours, 15 minutes.
- The flight landed in Auckland at 0340. After landing the flight crew noticed that there was a substantial amount of fuel still in the center tank, with minimal fuel in the main tanks, and that the center tank pumps were in the off position. The first officer recalled seeing an amber ‘fuel low pressure’ caution light flickering on while taxiing to the parking position and thinking it was probably associated with a main tank fuel pump.
- The captain recalled that the main tank fuel contents after landing were 750 kg in the left main tank and 950 kg in the right main tank (this flight was operated under EDTO rules and therefore had the auxiliary power unit (APU) running for the EDTO portion of the flight. The APU draws fuel from the left main tank and therefore a small imbalance in fuel after landing would have been expected). The Commission could not verify these figures as the captain requested that engineers transfer the fuel from the center tank to the main tanks in preparation for the aircraft’s next flight. The captain informed the duty line engineer and the maintenance watch duty engineer after shutdown that the aircraft had landed with 4000 kg in the center tank. The fuel log for the flight recorded total fuel on shutdown as 4640 kg.
- On 8 June 2022 the operator contacted Boeing (the manufacturer) to ask if a structural check of the aircraft was required due to its landing with this amount of fuel in the center tank. The manufacturer later responded that no check was required.
- The operator notified the Civil Aviation Authority (CAA) and the Australian Transport Safety Bureau (ATSB) of the occurrence on 9 June. The ATSB notified the Commission on 14 June. The delay between occurrence and notification meant the Commission was unable to access the cockpit voice recorder or the flight data recorder for the aircraft.
Personnel information
- The captain held a New Zealand Airline Transport Pilot Licence (Aeroplane) and a current Class One medical certificate. Their flying experience was 29,000 hours in total, with 10,000 hours on B737, of which 4500 had been with the operator. They also held a flight instructor rating and CAA Flight Examiner Approval (airlines nominate individuals who the CAA then assess to act as flight examiners and conduct pilot competency checks on behalf of the CAA for the renewal of pilots’ qualifications). The captain was nominated by the operator as the senior person for competency assessment.
- The first officer held a New Zealand Airline Transport Pilot Licence (Aeroplane) and a current Class One medical certificate. Their flying experience was 4500 hours total, with 700 hours on another variant of B737. They were under training as a new first officer with the operator, having had previous airline experience but two years away from flying due to COVID-19 restrictions.
- The flight crew reported for work at 1845 and had an active duty period of nine hours 40 minutes. Both pilots had been on rostered two days off on the days prior to the incident. The captain had completed three duties in the seven days preceding the incident and the first officer had completed two duties.
- Both pilots reported no health issues on the day of this flight. The first officer stated that they had been tired and having difficulty adapting their sleep patterns to night operations.
- The two pilots had flown together five days before the incident flight. That flight had been the unsuccessful check to line flight (check to line flight explained in footnote 5) for the first officer. Both pilots commented during their interviews that this had been discussed before the incident flight and they had agreed that the check flight outcome was correct and they were positive in moving forward together.

- The operator’s shorter flights from Auckland to Palmerston North or Christchurch would only have fuel in the main tanks. Flights from Auckland to Sydney or Melbourne would require additional fuel and therefore the use of center tanks.
- The manufacturer recommended that, when refuelling an aircraft, the fuel be distributed equally to the main tanks until they were full, and that any additional fuel be loaded in the center tank. The fuel-delivery system was arranged to draw fuel from the center tank before the main tanks. Each tank was fitted with check valves that regulated the output/flow pressure from the fuel pumps. The center tank check valves opened at a lower pressure than the main tanks’ check valves.
- For this process to work as designed, all fuel pumps associated with tanks with fuel loaded should be turned on as part of the FCOM Before start procedure. It is desirable for aircraft structural reasons to use the center tank fuel before the main tanks’ fuel, as having fuel in the center tank with no fuel in the main tanks increases the load forces on the wings.
- The FCOM states that if the center tank fuel quantity exceeds 453 kg (this equates to 1000 pounds (aircraft manufactured in the United States where imperial measures in use) and is stipulated by the manufacturer as a sufficient amount of fuel to minimise fumes in the tank and cover the pumps), the LEFT and RIGHT CENTER FUEL PUMPS should be switched on in the Before start procedure. The fuel log recorded that the fuel load prior to departure for the incident flight was 4520 kg in each main tank and 3980 kg in the center tank, totalling 13,020 kg.
Meteorological information
- The CAA is the International Civil Aviation Organization’s (ICAO’s) meteorological authority for New Zealand and is responsible for the provision of meteorological services (AIPNZ GEN 3.5, p. 1). Three providers are certified to supply various categories of meteorological service, and of these MetService (ibid, p. 2) has an exclusive licence to carry out the operational requirements prescribed in ICAO Annex 3, Meteorological Service for International Air Navigation.
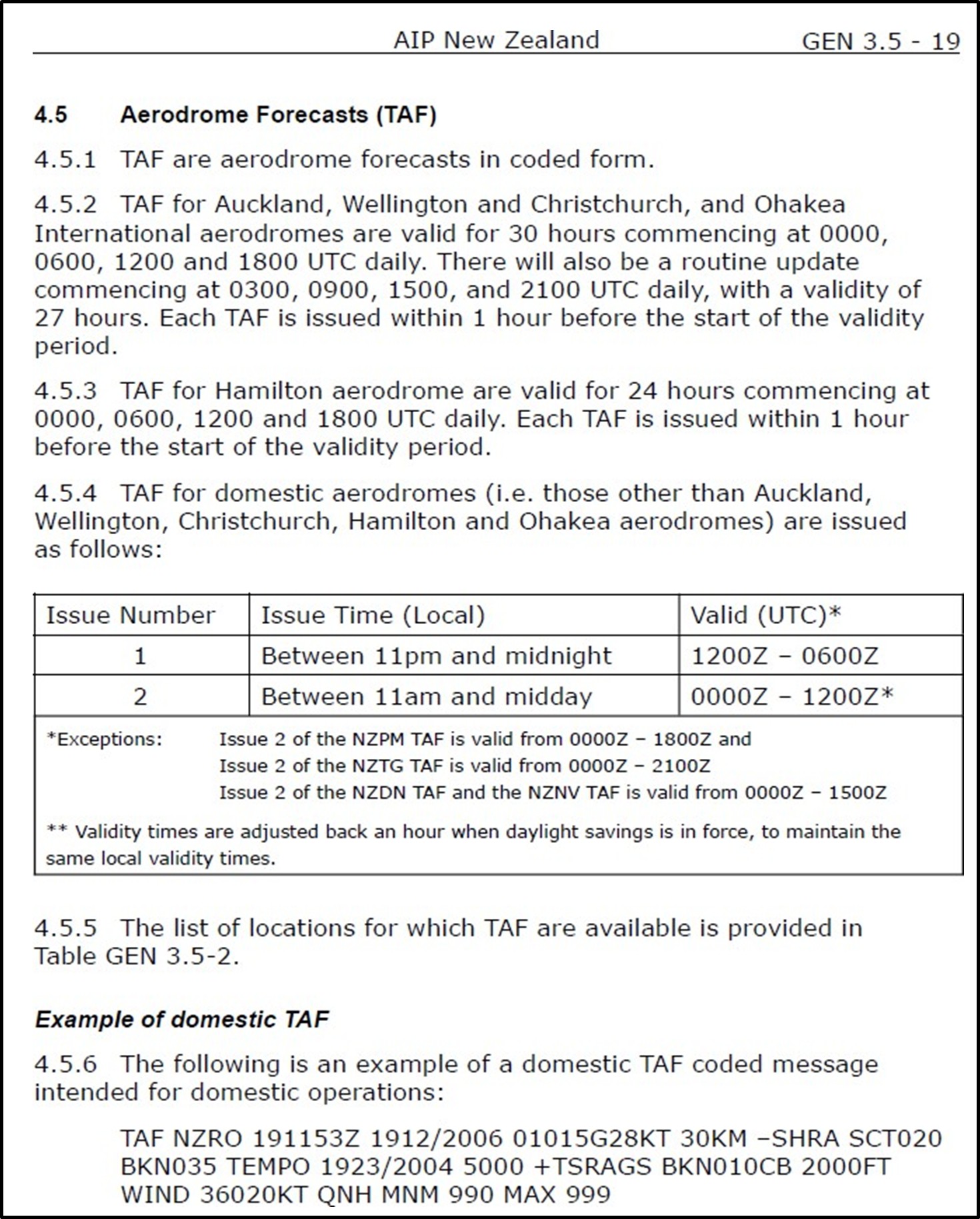
- Aerodrome forecasts are issued in coded form. For international aerodromes they are issued four times a day and provide forecasts for 30-hour periods. For domestic aerodromes the forecasts are issued twice daily with varying validity periods (ibid, p. 19).
-
The aerodrome forecast for Auckland that was issued to the flight crew at the preflight briefing was as follows:
NZAA 060509Z 0606/0706 03005KT 9999 -SHRA BKN030 PROB30 0615/0620 0500FG.
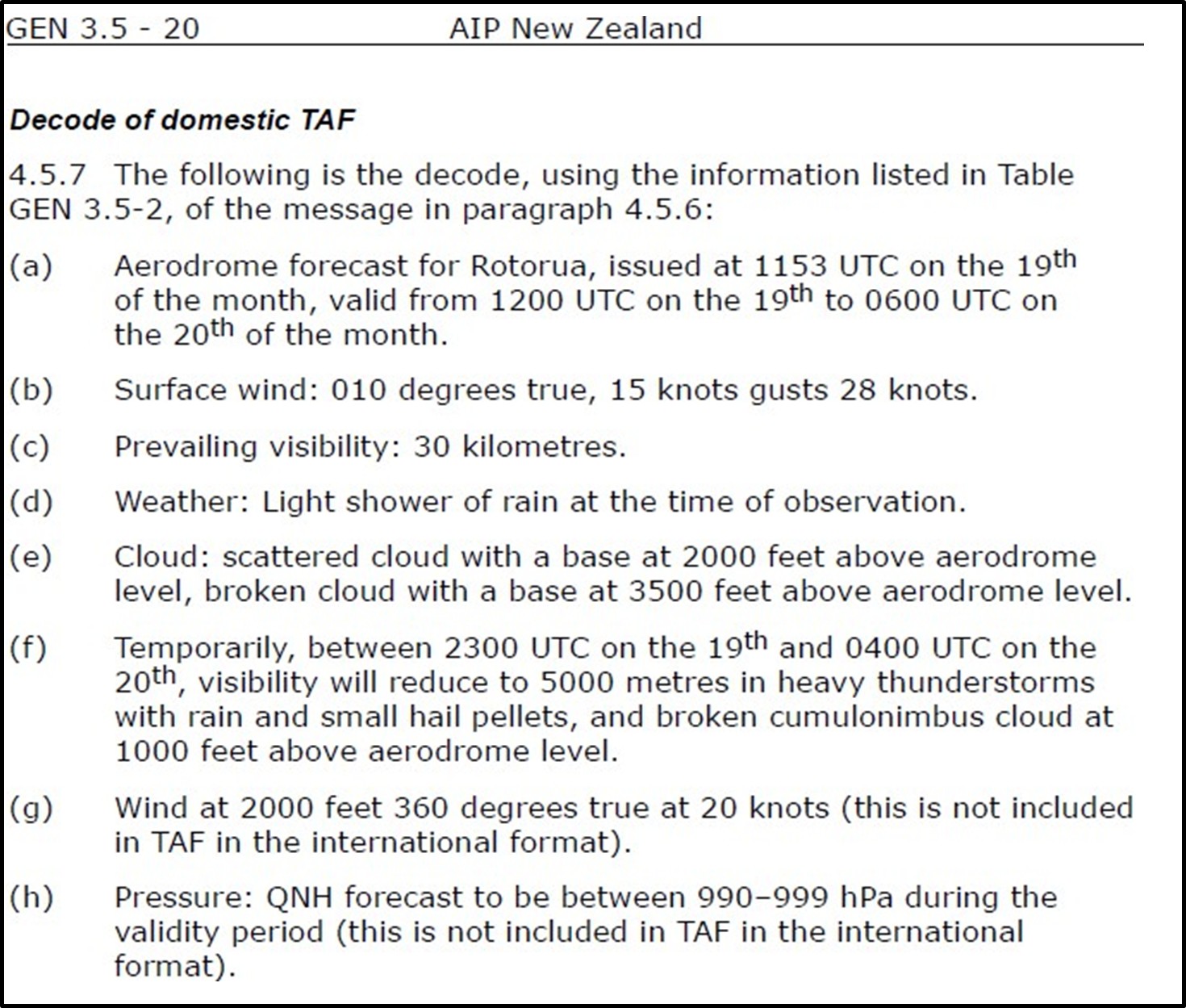
- A breakdown of this forecast is:
| NZAA | Auckland Aerodrome |
| 060509Z | the forecast was issued at 0509 UTC on the 6th of the month |
| 0606/0706 | the forecast was valid from 0600 UTC on the 6th until 0600 UTC on the 7th of the month |
| 03005KT | surface wind 030 degrees true, 5 knots [9.26 kilometres per hour] |
| 9999* | prevailing visibility in excess of 10 kilometres |
| SHRA | weather – rain showers |
| BKN030 | broken cloud with a base of 3000 feet [914 metres (m)] above the Aerodrome |
| PROB30 | from 1500 UTC until 2000 UTC there is a 30 per cent |
| 0615/0620 | chance of fog, with visibility reducing to |
| 0500FG | 500 m** |
*By convention, visibility is measured in metres or kilometres, while cloud base is measured in feet.
**The AWK2 scheduled time of landing at Auckland was 1555 UTC. The operator’s aircraft could not commence an approach to an airport with reported visibility less than 800 metres.
Organisational information
- The operator was a New Zealand CAA Air Operator Certificate (Airwork Flight Operations holds a New Zealand CAA Air Operator Certificate under CAR Part 119) holder based in Auckland and was part of Airwork Holdings Limited. Its business included commercial freight, heavy aircraft maintenance and international aircraft leasing.
- At the time of the incident the operator owned a fleet of 14 B737 aircraft, with seven aeroplanes in New Zealand (four based in Auckland and three in Christchurch), six aeroplanes at bases across Australia and one spare aeroplane. The New Zealand operation was predominantly night freight for three major clients.
- New models of the B737 are equipped with Aircraft Communications, Addressing and Reporting Systems (ACARS) (ACARS is a digital datalink system used in most airline aircraft for the transmission of short messages, and allows communication between airline and aircraft and for flight crew to obtain printouts of weather forecasts). However, to ensure consistency throughout the operator’s fleet, any aircraft with ACARS fitted had the unit removed before entering service. Pilots were therefore reliant on radio transmissions and satellite phones to send and receive information.
Extended Diversion Time Operations
- The operator’s flights across the Tasman Sea were based on EDTO. Historically, operators of twin-engine aircraft had to plan routes that kept their aircraft flight paths within 60 minutes’ flight time of aerodromes where they could land if they incurred serious malfunctions. As aircraft engines became more reliable, rules were developed to allow operations beyond the 60-minute limit and therefore allow more direct flight routing. In New Zealand this was covered by Civil Aviation Rules (CAR) Part 121, Subpart N EDTO Authorisation and Requirements.
- The EDTO rules in CAR Part 121 specify rigorous requirements for maintenance, aircraft checks, systems’ redundancy and allowable defects. The rules also apply more restrictive weather limits for an aerodrome to be suitable (an adequate aerodrome is one where the aircraft landing distance performance requirements at the expected landing weight can be met and appropriate aerodrome rescue and fire-fighting services are available, and there is at least one authorised instrument approach procedure. An adequate aerodrome becomes suitable when the weather minimum for the required type of use has been met; Airwork OCC Manual, 4.2 and 4.3) as an en-route diversion alternate when planning the EDTO segment of a flight.
- Maintaining and providing up-to-date weather and operational information for aircraft is also part of the EDTO rule requirements. Each operator is required to detail how it will implement this in its flight operations exposition to gain EDTO approval from the CAA (the regulator). The operator fulfilled this requirement through its Operations Manual and the OCC Manual.
- The operator’s Operations Manual stipulated that the OCC would provide pilots engaged in EDTO operations with flight planning and flight following, which included disseminating relevant weather and operational information. The manual also stated the experience and skills required of OCC staff. The OCC Manual gave more detailed information on the running of the OCC.
- The OCC was based in Auckland and managed the New Zealand and Australian flight operations. OCC staff provided flight planning and operational support to flight crew and operated on a 24-hour-a-day basis, with usually two staff covering night operations.
Flight planning
- Flight plans are required for all aircraft operating under Instrument Flight Rules, which include commercial operations (CAR 91.407). A flight plan includes the planned flight route and the nominated alternate, if required, and is submitted to the relevant air traffic service provider.
- For an EDTO flight, the EDTO alternates are also nominated on the flight plan, and the halfway point for the EDTO portion of the flight between these two alternates is stated. If an engine failure or decompression were to occur in the first segment of a flight, the flight would divert to the first EDTO alternate; after the halfway point the flight would continue to the second alternate. An important part of the flight plan is the calculation of the amount of fuel required for the flight should a failure and diversion be required at the most critical, or halfway, point. This is depicted in Figure 6.
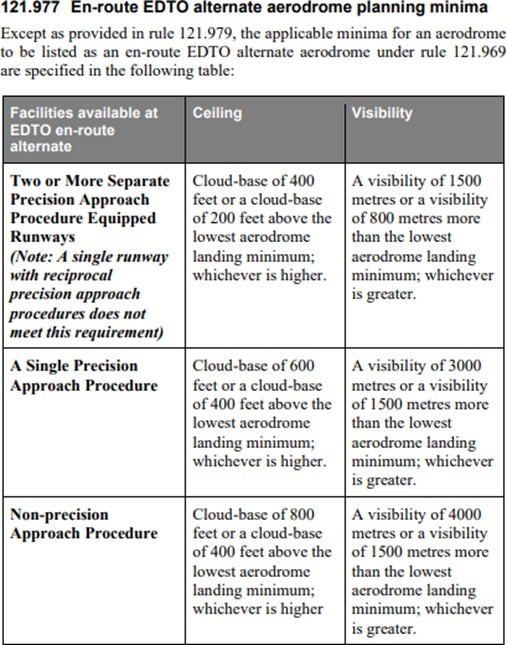
- To determine if an aerodrome is suitable to be nominated as an alternate, the weather forecast, ie the cloud base, visibility and wind, must be assessed. The other consideration is the types of navigation aids, and therefore instrument approaches that can be flown at the nominated alternate (CAR Part 121.977, shown in Appendix 3).
- The weather minima used at the planning stage are more restrictive than the aircraft operating minima. Using Auckland Airport as an example, there are a range of published instrument approaches that can be used for the two runways (05R and 23L). The alternate planning minima is the minimum acceptable weather for that airport to be nominated as an alternate and is predicated by the types of approach that are available. For Auckland, the cloud base must be forecast as a minimum of 600 ft above the aerodrome, and visibility of 3000 m or better. For comparison between the planning and operational stages, the limits for an instrument landing system approach to Auckland’s runway 23L (an instrument landing approach to runway 23L has the lowest minima requirements for this runway. It is termed a precision approach and provides both lateral and vertical guidance) requires a minimum cloud base of 200 ft and visibility of 800 m.
- The published approaches to Palmerston North Airport are based on navigational aids that do not provide the same accuracy as an of the instrument landing system approach, and are deemed as non-precision approaches. The weather forecast must be better than the Auckland example, with a minimum cloud base of 800 ft and visibility of 4000 m.
- The minima figures quoted above for Auckland and Palmerston North were published in the AIPNZ (AIPNZ Table ENR 1.5-7, p. 45) and were determined by applying CAR Parts 91.405 and 121.157 for alternate aerodromes and CAR Parts 121.969 and 121.973 for EDTO alternate aerodromes.
Safety management system
- An applicant for a grant of an airline air operator certificate must establish, implement and maintain a system for safety management (CAR 119.79). A safety management system (SMS) describes a systematic approach to managing safety, including the necessary organisational structures, accountabilities, responsibilities, policies and procedures (ICAO Doc 9859 Safety Management Manual, Fourth Edition, 2018). CAR Part 100.3 (see Appendix 3) outlines the requirements of an SMS, which include a process for risk management that identifies hazards to aviation safety, and safety assurance measures that ensure hazards, incidents and accidents are internally reported and actions are taken to prevent their recurrence.
Other incidents
- In 2007 the ATSB investigated a fuel-related event involving another operator’s Boeing 737-400 (ATSB report AO-2007-036). The incident flight was from Perth to Sydney, and in the cruise the master caution light and fuel low-pressure light illuminated, indicating low output pressure in the aircraft’s main fuel pumps. The flight crew identified that the center fuel pump switches remained in the OFF position and immediately selected them to the ON position.
- Relevant findings from the report covered the selection of fuel pump switches, the effective monitoring of switch selection, how switch selection is confirmed when completing checklists and the conduct of en-route fuel checks. Safety actions by the operator included a change to two checklists and procedures that required responses from both crew to some checklist items, and a reminder to flight crew to ensure that regular fuel-system configuration and consumption checks are performed during flight.
- The ATSB report referred to a search for similar events in the US National Aeronautics and Space Administration (NASA) Aviation Safety Reporting System. The search revealed six incidents in the period from 1994 to 2007 involving flight crew on B737 aircraft omitting to select the center tank fuel pumps ‘on’ during departure preparation and then not detecting this incorrect action during the Before start checklist.
- An updated search of this database was conducted by the Commission. It noted nine reported events of a similar nature in B737 aircraft in the period 1994–2023. The most recent report was from August 2006.
Analysis Tātaritanga
Introduction
- The standard procedure for B737 aircraft is to use fuel in the center tank before fuel in the two main tanks. Flight AWK2 flew from Sydney to Auckland and landed before the flight crew realised that fuel from the center tank had not been used.
- During the investigation of the fuel configuration event, it became clear that the operator’s systems to support the planning and operation of long-distance flights were not being applied as per the procedures described in its manuals.
- The following sections analyse the circumstances surrounding the event to identify those factors that increased the likelihood of the event occurring or increased the severity of its outcome. They also examine any safety issues that have the potential to adversely affect future operations. The first part of the analysis looks at the flight crew’s omission of not turning the center fuel pumps on and later sections review the operator’s operational procedures.
Center fuel pumps not turned on when required
Safety issue: The center fuel pumps were not switched on as required by the Before start procedure, and this omission was not captured by the crew completing the Before start checklist. If not detected, this omission has the potential to cause fuel starvation to the engines, increasing the risk of an accident occurring.
Checklist philosophy
- The sequence for preparing aircraft systems to commence a flight is detailed in the FCOM (relevant sections are included at Appendix 2). The FCOM details how each system should be prepared for each phase of flight, for example which systems need to be turned on prior to engine start, and who should carry out the action.
- One of the first officer’s tasks in the Before start procedure was to configure the fuel panel by selecting the fuel pump switches to ‘on’ (see Appendix 2). The procedure states that if the center tank fuel quantity exceeds 453 kg, the center fuel pumps should be switched on. In this instance the first officer turned on the main fuel pumps but omitted the center fuel pumps (see Figure 4 below for the fuel panel layout).

- The next task was to complete a checklist to confirm the completion of the actions required by the Before start procedure and that the aircraft was correctly configured. The operator used the industry-wide ‘challenge and response’ philosophy for checklists. This is detailed in the operator's Operations Manual and discussed below (see also Appendix 2).
- The Quick Reference Handbook (see Appendix 2) detailed who should conduct the checklist for each phase of flight; for example, the captain calls for the Before start checklist, the first officer reads the checklist and both pilots verify each item. On reading the Fuel checklist item, both the captain and the first officer were required to confirm the amount of fuel loaded and that the correct fuel pumps were on, before the captain responded with the fuel quantity in kilograms and pumps on. However, the flight crew did not identify that the fuel panel was incorrectly configured for the fuel load when completing the Before start checklist.
- The Before start checklist called only for a check of the fuel in kilograms and that the pumps were on. The checklist did not call for the pumps to be identified by the first officer or cross-checked by the captain. However, the Operations Manual Part A 3.13.2 gives guidance on challenge and response when using checklists, while the Quick Reference Handbook Checklist Instructions CI.1.1 states that both pilots are to ‘visually verify that each item is in the needed configuration or that the step is done’ (see Appendix 2).
- Fuel is loaded in the center tank when long flights require a large fuel quantity. For this operator that equated to flights across the Tasman Sea. Domestic flights were sufficiently short to not require fuel in the center tanks. The first officer’s previous flight had been a four-sector domestic trip, so the center tank did not have fuel in it for those sectors.
- Both pilots’ rosters for the two months before the occurrence were analysed to determine the split between domestic and Tasman flights. This showed that both pilots had operated more duties across the Tasman Sea than domestic flights, and therefore operated more often than not with fuel in the center tanks. The combination of the outbound sector of this duty requiring center tank fuel and the fact that the crew had operated more flights in the previous two months requiring center fuel than not led the Commission to conclude that recency bias had not influenced this occurrence.
- As mentioned in paragraph 2.47, the ATSB investigated a similar occurrence in 2007 (ATSB report AO-2007 036). In the resulting report it referred to a study conducted by NASA (Degani, 1990) following a series of accidents involving the improper use of checklists, checklist error and causes of checklist error. The study identified limitations in flight crew interactions with checklists, and among other recommendations suggested ‘the use of hands and fingers to touch appropriate controls, switches and displays while conducting the checklist’ as an effective enhancement for verifying the completion of checklist items. This suggested enhancement formed part of a safety recommendation in the ATSB report referred to in paragraph 2.47, and the operator in that incident responded that they would discuss the matter with the OEM (original equipment manufacturer) but had no intention of adopting the procedure at that time.
- Following the incident the captain reported that they had spoken to three fellow training captains employed by the operator, and that each had stated they had operated a recent flight where the center fuel pumps had not been switched on when they were required. Additionally, a notice to pilots was sent by the operator’s manager flight operations, implementing a change to the Before start checklist by adding ‘4/6 pumps on’ to replace ‘ pumps on’. The amended checklist had a specified response of ‘4/6 pumps on’ rather than a blank, and thus introduced a clear question with the two alternative responses as to whether four or six pumps were required to be turned on dependent on the fuel load.
Reduced turnaround time and curfew
- The late arrival into Sydney put pressure on the flight crew to complete tasks and be ready for their departure on the return sector prior to the government-mandated curfew. They were unsuccessful in obtaining updated weather forecasts for the return sector from OCC, as discussed in paragraph 3.46.
- The pressure was compounded when the flight crew requested pushback from ATC and were informed that there had been a change to the departure runway due to noise-abatement procedures. This interrupted the running of the Before start procedure and checklist as the flight crew was required to reprogramme the aircraft’s flight management computer with the new departure routing and recalculate the aircraft performance for take-off. There was also pressure to complete the tasks before the airport ceased all departures due to the curfew.
- Once the flight crew were ready, they again asked ATC for pushback. At this point the Before start procedure should have been completed, but the center fuel pumps were not turned on. The flight crew would have then carried out the Before start checklist, but they did not identify the omission. The first officer stated that the combination of the curfew approaching, fog forming in Auckland and the last-minute distraction of the runway change contributed to the omission.
Flight crew experience
- The captain was highly experienced and providing training for the first officer, who was an experienced pilot but new to this operator. The first officer was nearing the completion of their line training but had failed a line check on a previous flight with the training captain. This Auckland-Sydney-Auckland flight had been rostered for the first officer as support line training.
- There was the potential for a large authority gradient between the crew on these sectors given that the first officer had failed their line check on the previous flight with this captain. The captain reported that the previous check flight was discussed on the outbound sector and the first officer had been open to feedback. The first officer commented that they had been ok after failing the check flight and accepted that they needed a few more sectors to polish their performance.
- The captain was training on both sectors on this trip and therefore fulfilling their normal role as well as supervising the first officer in the completion of their tasks. This additional pressure, combined with a reduced turnaround time, the approaching curfew and the need to re-programme and replan the departure very likely led to the completion of the Before start checklist not capturing the omission.
Night duties
- Both pilots had had two rostered days off preceding this flight. In this instance the duty period commenced at 1845, and the initial incident happened approximately mid-way through the duty. Nevertheless, two-pilot night freight operations, with their unusual operating times, have the potential to increase crew fatigue levels.
- The captain had flown night operations with the operator for ten years and said they were well adjusted to night duties. The first officer said they had felt tired during this duty and that they had had difficulty adjusting to the sleep patterns required for night duties. They attributed the failed line check on their previous duty to their being tired and had taken one day of sick leave on the day after the line check. They had completed four duty periods in the 14 days preceding the incident flight, and all had been night duties. They had been rostered four days off prior to the incident flight.
- Both flight crew members stated that they had not felt the need to use controlled rest on either sector. The requirement to turn on the fuel pumps before engine start occurred mid-way through the duty and during a period of heightened workload. Reduced crew alertness levels were therefore unlikely to have been factors that contributed to the error.
En-route checks did not identify pumps not on
In-flight fuel check
- Pilots carry out fuel checks during flights to ensure they have sufficient fuel to complete the flights as planned and that fuel leaks have not occurred. The Operations Manual (Operations Manual Part A 5.8.2) stated that at appropriate waypoints the remaining fuel had to be recorded and evaluated to compare actual consumption with planned consumption, and that the remaining fuel had been sufficient to complete the flight with required reserves in place.
- The focus on this sector for the flight crew was obtaining weather reports, as there was a real possibility of their being unable to land at Auckland due to reduced visibility and then a subsequent diversion to Christchurch. OCC staff should have contacted the flight crew prior to the EDTO portion of the flight to advise them of any deterioration of weather at EDTO alternates, but as discussed in paragraph 3.48 the flight crew were not contacted.
- The flight crew attempted to obtain weather reports from VOLMET41 and by talking to other aircraft inbound to Auckland. There were two other aircraft inbound to Auckland: another of the operator’s flights from Melbourne (AWK82) and B767 Tasman Cargo Airlines (TMN2) (the ATC call sign of a flight operated by Tasman Cargo Airlines) from Sydney.
- The operator’s fleet of aircraft was not equipped with ACARS, as discussed in 2.34. The operator’s flight crew were therefore reliant on radio transmissions and satellite phone to send and receive information such as weather forecasts.
- As the flight approached Auckland, the flight crew of AWK2 were aware from monitoring ATC radio traffic and weather reports received from other aircraft that visibility was fluctuating. If the visibility reported by ATC had been less than the allowable minimum for their operation, they would not have been able to commence an approach and landing at Auckland (the operator has CAA approval to carry out Cat I approaches. These require a reported visibility, or runway visual range (RVR), of 550 metres or greater at the touch-down end of the runway. RVR is a measure of visibility reported by ATC). Over the ATC radio they heard the preceding aircraft (TMN2) fly a go-around due to the reducing visibility, and TMN2 was then sequenced to fly a second approach before AWK2. TMN2 flew a second approach and go-around and entered a holding pattern before diverting to Christchurch, whereas AWK2 was able to complete a successful approach and landing as the visibility fluctuated.
- Commission investigators obtained a copy of the flight plan used by the flight crew. Several fuel checks were annotated. The captain recalled that they had carried out en-route fuel checks against the flight management computer and not the fuel gauges, as was their normal practice (Figure 5 shows the flight management computer located on the centre console, with fuel gauges directly above). The Operations Manual stated the actions required to carry out a fuel check but did not mention fuel distribution.
- En-route fuel check guidance from another operator stated that a fuel check should ensure that the calculated fuel on board is correctly balanced and distributed. Had the flight crew included fuel gauges as part of the fuel checks, it is likely they would have noticed that fuel quantity in the center tank was the same total as when they had departed, and by implication the center pumps were off.

More recent aircraft variants
- More recent variants of the B737 and subsequent aircraft, such as the Boeing 757 and Boeing 767, have included an engine indication and flight crew alerting system called EICAS. One of its functions is to monitor aircraft systems and configurations, including when fuel is loaded into a center tank. Should a flight crew not turn on the center tank pumps prior to engine start when required due to the fuel load, a caution message is generated to alert them.
Potential go-around
- The weather in Auckland was fluctuating as AWK2 approached, and a diversion was a real possibility. One hour before AWK2 landed, the reported visibility was 275 m (the runway visual range reported in this instance by ATC via the Automatic Terminal Information Service), which was below the operator’s minimum and would have prevented the flight crew commencing an approach. As detailed in paragraph 3.26, another operator’s aircraft flew two go-arounds due to the weather prior to the approach flown by AWK2 and finally diverted to Christchurch.
- At the time AWK2 commenced the approach, the visibility was still fluctuating but above the required minimum, and as a precaution the crew briefed for and conducted an autoland. If AWK2 had subsequently flown a go-around from this approach due to the low visibility, fuel consumption would have increased rapidly because of the engines’ high power demands. The fuel on shutdown was noted in paragraph 2.12 as 4640 kg, and with 4000 kg reported in the center tank that left 640 kg in the main tanks. The operator advised that the guidelines for B737 stated that 640 kg would be used for a go-around and further approach. Consequently, it is very likely that during a go-around manoeuvre the master caution light and fuel low pressure light would have activated as fuel in the main tanks neared exhaustion.
- In this scenario there was no checklist or procedure that would have directed the flight crew to turn on the center pumps, as checklist logic (normal and non-normal checklists assume that all procedures have been carried out as per the manuals, so in this instance the assumption of any checklist would have been that center fuel had already been used) would have assumed that the center fuel had already been used. It would have required the flight crew to analyse the situation and determine that fuel was available in the center tank, which would have been challenging given the high workload of flying a go-around and possible diversion. Therefore, there would have been a very real potential for an engine failure if a go-around had been required. The captain had recognised this and commented that “the risk that we put ourselves in by not turning those pumps on was that had we have had to do a go-round we’ve put ourselves in a situation that may have been critical”.
Departed without suitable alternates nominated
- Flight planning is discussed in paragraph 2.40, specifically the requirement to nominate a destination alternate and EDTO alternates for each flight. At the planning stage, the nominated destination alternate for AWK2 was Palmerston North and the second EDTO alternate was Auckland. The weather forecasts for both aerodromes at the planning stage were suitable.
- Just prior to AWK2’s landing in Sydney, new weather forecasts were issued by MetService for New Zealand airports. These showed a deterioration in the weather. The original forecasts for Auckland obtained at the briefing had shown a 30 per cent probability of fog. The new forecast for Auckland predicted fog present rather than possible, and reduced visibility at Palmerston North and Christchurch.
- From a planning perspective, Palmerston North no longer met the requirements for nomination as a destination alternate for Auckland, and neither did Christchurch. Auckland, Christchurch and Palmerston North also did not meet the requirement for nomination as EDTO en-route alternates.
- The weather forecast for Wellington was suitable for it to be used as a destination and EDTO alternate. However, had an aircraft been diverted there it would have remained on the ground until 0600 due to local curfew restrictions. It would also have meant no custom and immigration staff to process the flight crew and no loaders to move cargo if required.
- On landing in Sydney, the flight crew were notified by email that fog was then forecast for Auckland. The flight crew attempted to get updated weather forecasts and reports for the return sector from the OCC via satphone, but they stated that the person they spoke to was unable to decode the weather forecast and relay it to the flight crew in an understandable format.
- The flight crew responded to the email, requesting that flight plan fuel be increased to 13,000 kg, thus adding 1000 kg (adding 1000 kg to the total fuel would have given the crew additional flexibility. For example, they would potentially have had enough fuel to fly to Auckland and then divert to Christchurch). The flight crew did not request a new flight plan to indicate a change in nominated destination alternate and EDTO alternates, nor were they offered one by the OCC. In addition, neither the flight crew nor the OCC considered nominating Wellington as an EDTO alternate or undertook any fuel calculations in support of this.
- EDTO authorisations and requirements, laid out in CAR Part 121 Subpart N, are in place to provide a high level of safety for twin-engine aircraft operating on extended-range routes. The intent of the rules is to avoid diversion, but also to ensure a safe outcome should a diversion be required.
- The flight plan that was originally submitted for this flight nominated Sydney and Auckland as the EDTO alternates. It calculated the equal time point (ETP) for the EDTO critical fuel scenario and provided the geographical coordinates of the point.
- Figure 6 shows the EDTO planned routing. The yellow line depicts the flight as planned with Sydney and Auckland the EDTO alternates. The EDTO entry point is depicted as EEP1 and is the entry point to the EDTO portion of the flight, which is 60 minutes out from the departure point. The EDTO exit point is depicted as EXP1 and is the exit point from the EDTO portion of the flight, which is 60 minutes’ flight time to the destination. If Auckland had been unsuitable and Wellington nominated as the EDTO alternate, the ETP between the EDTO alternates of Sydney and Wellington (depicted in red) would have moved from the original point. This would have required more fuel as the fuel usage would have been higher on the ETP to the Wellington sector as it was longer then ETP to Auckland.

- Flight AWK82 was another company-operated B737 inbound from Melbourne on that evening. It landed in Auckland at 0346, six minutes after AWK2. The flight plan for this flight also nominated Palmerston North as the alternate and Auckland as the second EDTO alternate.
- The two operators’ flights departed Sydney and Melbourne for Auckland with sufficient fuel to complete their flights, but with flight plans nominating destinations and EDTO alternates that did not comply with regulatory or company flight planning requirements. The flight crew had no means to accurately determine an ETP to a suitable EDTO alternate. The safety buffer that the EDTO ruleset normally provided was reduced.
OCC staff not providing support to flight in accordance with operator’s exposition
Safety issue: The OCC staff did not provide flight support in the form of updated weather forecasts for aerodromes or flight plans in accordance with the operator’s exposition. The absence of current and relevant information can affect a flight crew’s performance and the safety of a flight.
- As discussed in paragraph 2.35, EDTO is regulated under CAR Part 121 Subpart N. The operator stipulated how it would meet the requirements of Subpart N by outlining the duties and activities of the OCC in the operator’s Flight Operations Exposition OCC Manual.
- The OCC Manual outlined the functions of the OCC, which included flight planning and flight following. These required OCC staff to review NOTAMs and weather forecasts and prepare and submit flight plans for the operator’s flights. OCC staff also provided updated information in support of pilot-in-commands’ responsibility for operational control once flight plans have been released (OCC Manual, Section 1.3.1).
- On landing in Sydney, the flight crew received an email from the OCC advising that the weather was deteriorating at Auckland for the return sector. However, they were not provided with updated forecasts for destinations or potential alternates. Both pilots stated that when they contacted the OCC while on the ground in Sydney, the person they spoke to had difficulty decoding the weather forecast and giving them the information they required. They advised the OCC by email that they required an extra 1000 kg of fuel but they did not request or receive an amended flight plan to reflect the increased fuel load or a change in nominated alternates.
- EDTO flight watch is also described in the OCC Manual (OCC Manual, Section 6.17). Among other tasks is a requirement for OCC staff to contact the flight crew as the aircraft approach’s EDTO entry points to notify them of any changes in weather or aerodrome conditions that may affect the suitability of nominated EDTO alternates.
- This contact between aircraft and the OCC as part of flight watch is via satphone and is recorded on an EDTO flight sheet; an example of the sheet is included in the OCC Manual (OCC Manual, Section 6.18). The OCC manager confirmed that the log for the night of the incident flight had not been filled out. The Commission sighted this document. The flight crew confirmed that they had not been contacted by OCC via satphone.
- The process for OCC staff to obtain updated weather forecasts was manual and required reviews of email accounts. The OCC manager acknowledged that, at that time, system issues meant OCC staff could not do flight watch as effectively as the manager would have liked. The OCC manager also said that their main challenges had been to find suitably qualified people to work in the OCC and for the OCC to be fully staffed.
- The support given to flights AWK2 and AWK82 by OCC staff on the evening of the incident did not meet the requirements stipulated in the approved manuals. OCC staff did not provide relevant and timely weather information, and the flight plans were not updated. This reduced the enhanced safety requirements of the EDTO ruleset.
Flight crew responsibility
Safety issue: The flight crew on the operator’s two flights (AWK2 and AWK82) on 7 June departed Auckland with flight plans that did not comply with the operator’s or the regulator’s alternate and EDTO fuel and planning requirements. Flight crew need to ensure that their flights are compliant with the relevant requirements to help them ensure flights are conducted as safely as possible.
- A flight plan calculates and records fuel requirements for flight to a destination and then on to an alternate. It also assesses the EDTO critical fuel scenario and calculates the fuel required from the most critical point of the flight to the EDTO alternate should a failure occur at the most critical point. It is important that flight crew have accurate information so they can make good decisions in the event of failures.
- The pilot-in-command of an aircraft is ultimately responsible for ensuring that their submitted flight plans meet company and regulatory requirements.
Regulatory oversight
Safety issue: The regulator’s oversight and auditing of the operator identified deficiencies in the operator’s safety management system that have yet to be fully addressed. The regulator has a role in ensuring that deficiencies in an operator’s safety management system are addressed to reduce the risk of accidents occurring.
- As described in the preceding paragraphs, the inquiry identified deficiencies in the operator’s flight planning and the OCC’s support for flights. Other issues around documentation control in the operator’s quality assurance systems were also identified. The training record of the first officer’s previous check to line flight could not be located by the operator. Errors in updates to the OCC Manual were also noted by the Commission. These were reported to the operator and investigated, and a clerical error in the update process was noted and rectified. The operator has recently appointed a documentation quality control manager to oversee and review document control.
- The regulator has stated that it takes a risk-based approach to reduce the regulatory burden for those with good-quality safety systems (CAA Briefing (May 2024); email briefing to subscribers on 30 May 2024). Its policy on an intelligence-led, risk-based regulatory approach is detailed in a document, Regulatory Safety and Security Strategy 2022-2027, which explains aviation risks and the prioritisation of effort. The regulator is reliant on the SMS of an operator to identify areas that could signal or lead to hazards and risks.
- As part of this inquiry, recent regulator audit reports on the operator were reviewed. The CAA report for CAR Part 119 Operational Recertification in March 2019 stated that some elements of the SMS had progressed since its original approval in 2017, while others had not. Subsequent audits in 2021 and 2022 highlighted other deficiencies with the operator’s SMS. These findings included that risks identified in internal audits and investigations were not being fed back into the safety and risk management process. The regulator also commented that the turnover of senior management meant that envisaged improvements had not come to fruition.
- The Commission reviewed documentation provided by the regulator to support the interactions with and the significant work programme undertaken by the operator and overseen by the regulator as they work to resolve the deficiencies identified. The regulator stated that ‘this is work in progress given the complexity and range of problems identified and the fixes required’. The regulator confirmed that the operator’s SMS was not yet fully effective.
- ICAO guidance on SMS acknowledges that ‘safety management takes time to mature and the aim should be to maintain or continuously improve the safety performance of the organization’ (ICAO Doc 9859, Safety Management Manual, Fourth Edition, 2018, 1.3.4.3). It goes on to say that ‘the relationship between a State and its service providers should evolve beyond compliance and enforcement, to a partnership aimed at maintaining or continuously improving safety performance’ (ibid, 8.3.4.4). The objective is for an operator’s SMS to mature from operating to being effective.
Appendix 1. Weather forecasts
Aerodrome forecasts (TAF) issued on 5/6th June 2022 by MetService
(decode information on following page from AIP (AIP GEN 3.5, p. 19 & 20))
Forecasts used for flight crew’s original briefing:
TAF NZPM 052312Z 0600/0618 VRB02KT 20KM BKN050
TAF NZAA 060509Z 0606/0706 03005KT 9999 -SHRA BKN030 PROB30 0615/0620 0500 FG
TAF NZCH 060509Z 0606/0706 VRB02KT 9999 FEW050 PROB30 0610/0616 0500 FG BECMG 0616/0618 04010KT
Forecast issued prior to flight AWK2 departure from Sydney:
TAF NZCH 061109Z 0612/0712 VRB02KT 2000 BR FEW05 TEMPO 0612/0616 0500 FG BECMG 0616/0618 04010KT 9999 NSW FM070600 04005KT 9999 -RA BKN050
TAF COR NZCH 061120Z 0612/0712 VRB02KT 2000 BR FEW050 TEMPO 0612/0616 0500 FG BECMG 0616/0618 04010KT 9999 NSW FM070600 VRB02KT 9999 -RA BKN050
TAF NZAA 061138Z 0612/0712 03008KT 0500 FG BKN012 BECMG 0612/0614 BKN003 BECMG 0620/0622 9999 NSW FEW006 SCT025 TEMPO 0710/0712 6000 SHRA
TAF NZPM 061138Z 0612/0706 VRB02KT 2000 BR FEW075 TEMPO 0612/0621 0500 FG BECMG 0620/0622 25KM NSW
ATIS for NZAA
1408Z ATIS G: ILS DME Cat3 23L Dry 310/4 800m FG RVR TD 1000 MP 900 SE 650 VV500’ 10/10 1015
1427Z ATIS H: ILS DME Cat3 23L Dry VRB/1 800m FG RVR TD 275 MP 350 SE 1000 VV300’ 11/11 1015
1513Z ATIS I: ILS DME Cat3 23L Dry VRB1 1000m FG RVR TD 900 MP 1000 SE 550 FEW002 11/11 1015
15:33 ATIS J: ILS DME Cat3 23L Dry 080/3 700m FG RVR TD650 MP 650 SE 1500 FEW002 11/11 1015
Appendix 2. Airwork Checklists
Airwork NZ Boeing 737-300/ -400 Flight Crew Operations Manual (FCOM), Revision 19, Pg NP.21.32


Airwork Operations Manual Part A General Procedures, Amendment 1, Pg 3-10

Airwork 737 Quick Reference Handbook, Revision 19, Pg NC.1

Airwork 737 Quick Reference Handbook, Revision 19, Pg CI.1.1

Appendix 3. Civil Aviation Rules (CARs)