TAIC report presents rail safety issues with working practices, engineering protections, and safety guidelines - factors that contributed to unintended shunt movement, in Picton. A remote-controlled shunt loco and wagon moved off the end of the quay-to-ferry rail linkspan and into the harbour.
Factual information Pārongo pono
West rail yard, Picton
- The Picton freight yard facility and rail linkspan structure are strategic assets in connecting State Highway 1 and the North Island Main Trunk to the South Island. It is a vital part of New Zealand’s transport and tourism infrastructure.
- The west rail yard at Picton consists of seven designated railway tracks (see Figure 3), also referred to as ‘roads’ in rail terminology.
- Roads 1 to 6 are used for general shunting and road 19 is used for storing surplus rail wagons.
- Freight trains enter the yard on the main north line from the south. The port and rail linkspan are situated at the north end of the yard.

Narrative
- At 0600 (times in this report are in New Zealand Standard Time and expressed in the 24-hour mode) on 1 September 2021, a two-person shunt team consisting of a remote-control operator (RCO) and a rail operator (RO) commenced duty at the Waitohi Picton KiwiRail freight depot.
- The RCO was issued with an Arataki 1 remote-control pack (see Figures 4 and 8) and configured shunt locomotive6 DSJ4004 (the shunt locomotive) for remote operations.
- Due to rail ferry scheduling disruptions, the shunt team was informed by the acting team leader that the day’s tasks would likely differ from those normally expected.
- At 0605 all the prescribed checks on the shunt locomotive had been completed, including a mandatory brake test.
- Between approximately 1100 and 1300 the shunt team was able to take the second break of the shift. Before stopping work the RCO secured the shunt locomotive by chocking its wheels, shutting it down and deactivating the remote-control pack.

- During the course of the morning KiwiRail operations advised the Picton acting team leader that the rail ferry Aratere would be arriving that evening. On completion of their break the shunt team began preparing for the vessel’s arrival.
- After completing a shunting movement, the RCO stopped the shunt locomotive at the north end of west 4 road and waited for the arrival of KiwiRail Train 736 (Train 736).
- The RO, who had been working with the RCO, left the RCO and relocated to the south end of the yard in preparation for the arrival of Train 736. The RO remained at the south end of the yard to couple two freight locomotives to a freight train while the RCO carried out their tasks at the north end of the yard.
- At 1520 Train 736 arrived in the Picton yard. The acting team leader contacted the RCO using an ultra-high frequency (UHF) radio and instructed the RCO to find a refrigerated wagon that was part of Train 736.
- The RCO positioned themselves on board the shunt locomotive and commenced moving it along west 4 road adjacent to Train 736. Unable to locate the refrigerated wagon, the RCO stopped the shunt locomotive before reversing north to locate the head wagon, IH7430, instead. The head wagon was on west 2 road and was carrying two empty hazardous goods containers and needed to be taken to the container transfer terminal (CTT) (see Figure 7, pictures 1–2).
- On arrival at west 2 road, the RCO connected the shunt locomotive to the head wagon.
- Initially the RCO was going to take the head wagon from west 2 road to the CTT along west 4 road, but after entering west 4 road the RCO stopped the shunt locomotive and decided it would be quicker to move to the CTT along west 6 road (see Figure 7, picture 3).
- Changing the route meant the RCO needed to move the shunt locomotive north along west 4 road and then towards the rail linkspan, before stopping to set number 55 points manually towards west 6 road (see Figure 7, picture 4). Once the points were set, the RCO could travel south and enter west 6 road and head towards the CTT.
- When the RCO stopped the shunt locomotive to set number 55 points manually, they started walking towards the points, but it became apparent that the head wagon was fouling them. For the RCO to clear the fouled points, the head wagon needed to be moved approximately 30 centimetres north, towards the rail linkspan (see Figure 5).

- With the shunt locomotive stopped, the RCO started walking south towards the number 55 points lever (see Figure 7, picture 5). They then took their mobile phone out of their pocket, intending to call the CTT to inform them that they were running late, before remembering that the use of mobile phones was prohibited and so placing the phone back in their pocket.
- Tranzlog (the data-recording system fitted to the shunt locomotive)11 showed that at 1529:27 the brakes were released using the remote-control pack. This was followed by a throttle commanded to notch one12, which started the shunt locomotive moving north to clear the fouled points, towards the rail linkspan (see Figure 6). As the shunt locomotive started moving north, the RCO continued walking south, facing away from the shunt locomotive and listening to a conversation on the UHF radio.
- At 1529:35 the throttle was moved from notch one to notch two, which increased the speed to 10 kilometres per hour at 1529:52 and 13 kilometres per hour at 1530:01, when the throttle was moved back down to notch one.
- At 1530:13 the throttle was moved again, putting the locomotive into idle.
- Each of the throttle movements reset the vigilance system13 and delayed an automatic braking response.

- After the brakes were released and the throttle activated, the shunt locomotive travelled a distance of 112.5 metres, traversing an unprotected road vehicle crossing and entering the rail linkspan.
- During this time the RCO continued walking south away from the shunt locomotive’s northerly direction of travel. By the time the RCO turned around, the shunt locomotive and wagon were on the rail linkspan (see Figure 7, picture 6).
- The shunt locomotive was travelling at 3 kilometres per hour when it entered the raised portion of the rail linkspan, at 1530:19.
- As the shunt locomotive travelled up and along the unsupported rail linkspan, its weight caused the rail linkspan to drop towards the harbour.
- The acute angle between the shunt locomotive and the attached head wagon caused the shunt locomotive and wagon to separate. The brake hoses uncoupled (disconnected from each other) and the pressurised air vented to the atmosphere. The loss of air pressure caused the shunt locomotive’s emergency brakes to apply.
- This emergency brake application occurred too late to stop the momentum of the shunt locomotive taking it over the edge of the rail linkspan, entering Picton Harbour and sinking immediately.
- The two empty hazardous goods containers loaded onto the head wagon provided enough buoyancy to keep the head wagon afloat once it entered the water.

Key personnel information
- The RCO had joined KiwiRail in 2011, initially as an RO. They had successfully completed the RCO practical mastery test on 28 April 2021 and had received certification for RCO duties four months prior to this incident.
- The RO had joined KiwiRail in 2019 and been certified as an RO on 9 July 2020. The RO’s duties included assisting the RCO in shunting operations by coupling wagons and ensuring routes were clear for shunt locomotives to move safely.
- The acting team leader was also a certified RO, with four years’ experience in that role. They had started relieving as team leader at Picton about five weeks prior to the incident.
The Arataki 1 remote-control pack
- An image of the Arataki 1 remote-control pack can be seen in Figure 8. It is fitted with a vigilance system that, when turned on, sounds an audible alarm if there is no controller activity for 27±1 seconds. After 34 seconds it initiates emergency braking.
- The red mushroom emergency stop button is located on the display panel, at the right-hand side when in the harness. When the emergency stop button is pressed, the throttle returns to idle and the emergency braking is applied.

- The pack is fitted with a prevention mechanism function to make it ‘safe’. It turns off a remote-control key fitted to the side of the unit, and as a result the pack is bypassed, and the locomotive’s brakes are applied to prevent any uncontrolled movement.
Recorded data
Train data recorder
- The Tranzlog data unit was recovered from the locomotive after it had been submerged in approximately 10 metres of seawater for almost three days. Overseen by TAIC investigators, the unit was sent to the manufacturer for inspection and data recovery.
- The recovered data was used by the Commission in its analysis of this incident.
CCTV
- A closed-circuit television (CCTV) recording, taken by a security camera fitted near the south end of west rail yard at Picton, was recovered following the incident. The recording allowed investigators to observe the incident as it unfolded and assisted them in confirming the hypothesis of why the incident occurred.
Site and salvage information
- Due to a quick response from Port Marlborough, including from the oil spill response team who surrounded the site with spill-containment equipment and absorbent booms, the impacts on the environment were kept to a minimum.
- The 52-tonne locomotive and the wagon were recovered using two 300-tonne cranes. The salvage operation took three days and cost in excess of $500,000.
- Additionally, the weight of the locomotive travelling along the unsupported rail linkspan caused the rail linkspan to collapse and drop into the water. This in turn caused extensive damage to the rail linkspan.
Meteorological information
- On the day of the incident the weather was fine with light winds and visibility was good.
Organisational information
- KiwiRail Holdings Limited (trading as KiwiRail) is a New Zealand state-owned enterprise responsible for rail operations in New Zealand. It also operates the Interislander rail ferry.
- KiwiRail also provides infrastructure and engineering services for maintaining and improving the rail and ferry networks.
- Port Marlborough owns and maintains the ferry terminal assets, including the rail linkspan and infrastructure at Picton.
Remote-control operator training and certification
Overview
- To operate remote-control locomotives, rail personnel must have certification for shunting duties. The certification is intended to give them skills to carry out the shunting and related operating duties commonly found in commercial rail operations.
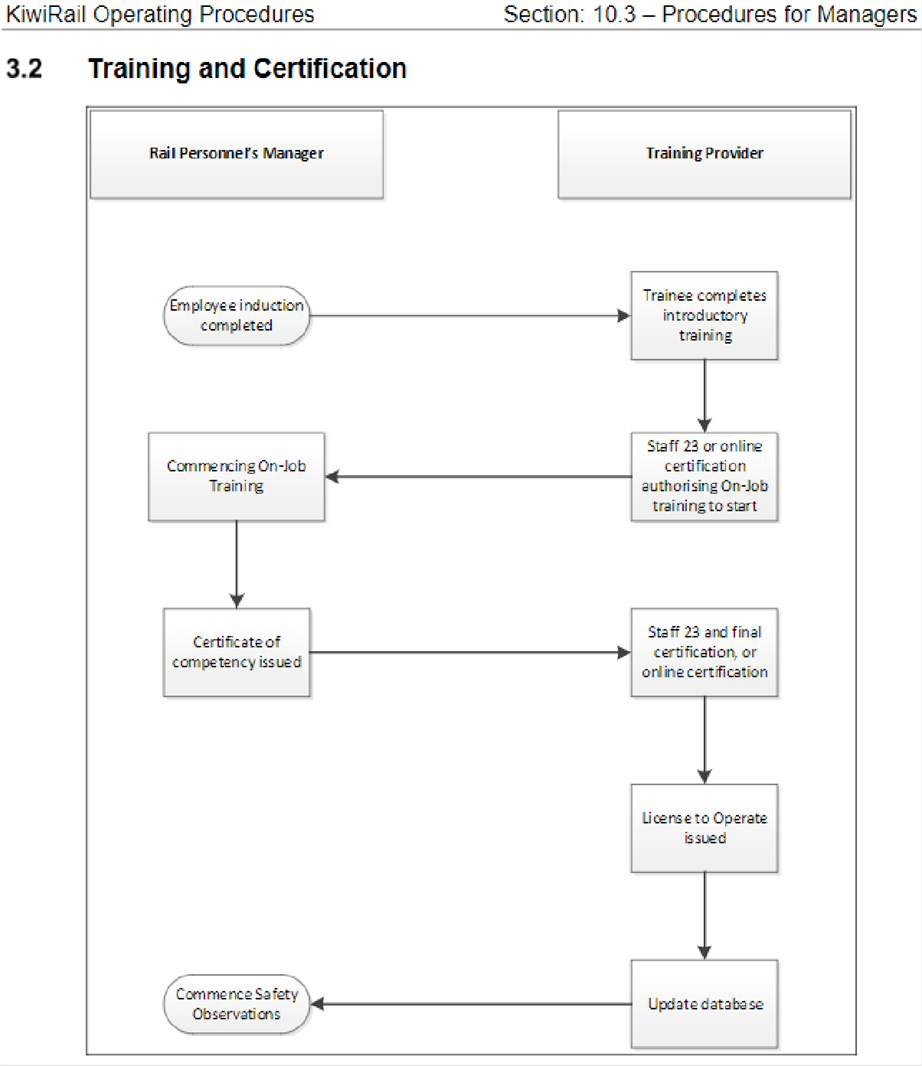
- After successfully completing the initial theory training, students undertake a period of on-the-job training (OJT).
- After OJT, the students must pass practical assessments and mastery tests to confirm their skills.
- The students also receive training that enables them to control locomotives manually during shunting within designated yard boundaries and in emergencies, such as clearing a main line when a remote-control pack is defective.
- Practical OJT includes a minimum 30 hours’ use of a remote-control pack and 10 hours’ manual operation of a locomotive.
- All training is provided by KiwiRail’s learning and development team.
Qualifications of the Picton RCO
- The RCO had successfully completed the initial theory training at Picton in March 2021, and on completion commenced OJT.
- When they had satisfactorily completed their OJT, the RCO had requested, and received, an additional week of training dedicated to operating the shunt locomotive in manual mode.
- On 28 April 2021 the RCO had been assessed by a KiwiRail assessor and certified to perform the role of RCO.
Rail personnel support process
-
KiwiRail Operating Procedures, Section 10.3 – Procedures for managers, rule 5.3.6 stated in part:
the purpose of the rail personnel support program for new rail staff is to support them to attain levels of competency that will assist them in achieving the required operating standards.
- The support programme included a requirement to: conduct safety observations; undertake Tranzlog data analysis to monitor driver behaviour; and complete theory tests.
- The safety observations were required to be conducted once a month for the first four months, followed by one further safety observation in the following three-month period.
- The successful completion of the support programme resulted in rail personnel returning to normal safety observations, conducted once every eight months.
- The RCO involved in this incident had not undergone any safety observations since becoming certified four months prior to this incident.
Other information
- The rail linkspan was designed to connect the rail ferry Aratere to the rail line at the Picton ferry terminal and facilitate the discharge and loading of rail vehicles.
- As the rail linkspan is lowered, it locates a central pin into an eye on the stern of the vessel. This ensures that the rail tracks inside the vessel are lined up correctly with the rail tracks on the rail linkspan.
- The rail linkspan is attached to large concrete weights by cables and pulleys on each side that allow it to be raised and lowered in a controlled manner. When it is not in use, the rail linkspan is held safely on wires and counterweights.
- The rail linkspan is maintained by Port Marlborough.
- The security gate was designed to restrict entry to the rail linkspan when it was not in use. The security gate was open at the time of the incident.

Tests and research
Testing the remote-control pack
- The remote-control pack, including the original battery, was taken to the KiwiRail Hutt Workshops for examination. A Commission investigator witnessed the examination.
- When the remote-control pack was powered up, all functions and controls were tested and found to be working in accordance with the instructions outlined in the KiwiRail Rail Operating Code (ROC), Section 5.2 for remote-control locomotives.
Radio communications and emergency calls
- The shunt operations team at Picton used portable UHF radios for communication.
- UHF radio is also used to send automatic emergency calls to train control (train control is situated in Wellington and is responsible for track authorisations and the safe movement of rail traffic) when an emergency stop button on a remote-control pack is activated.
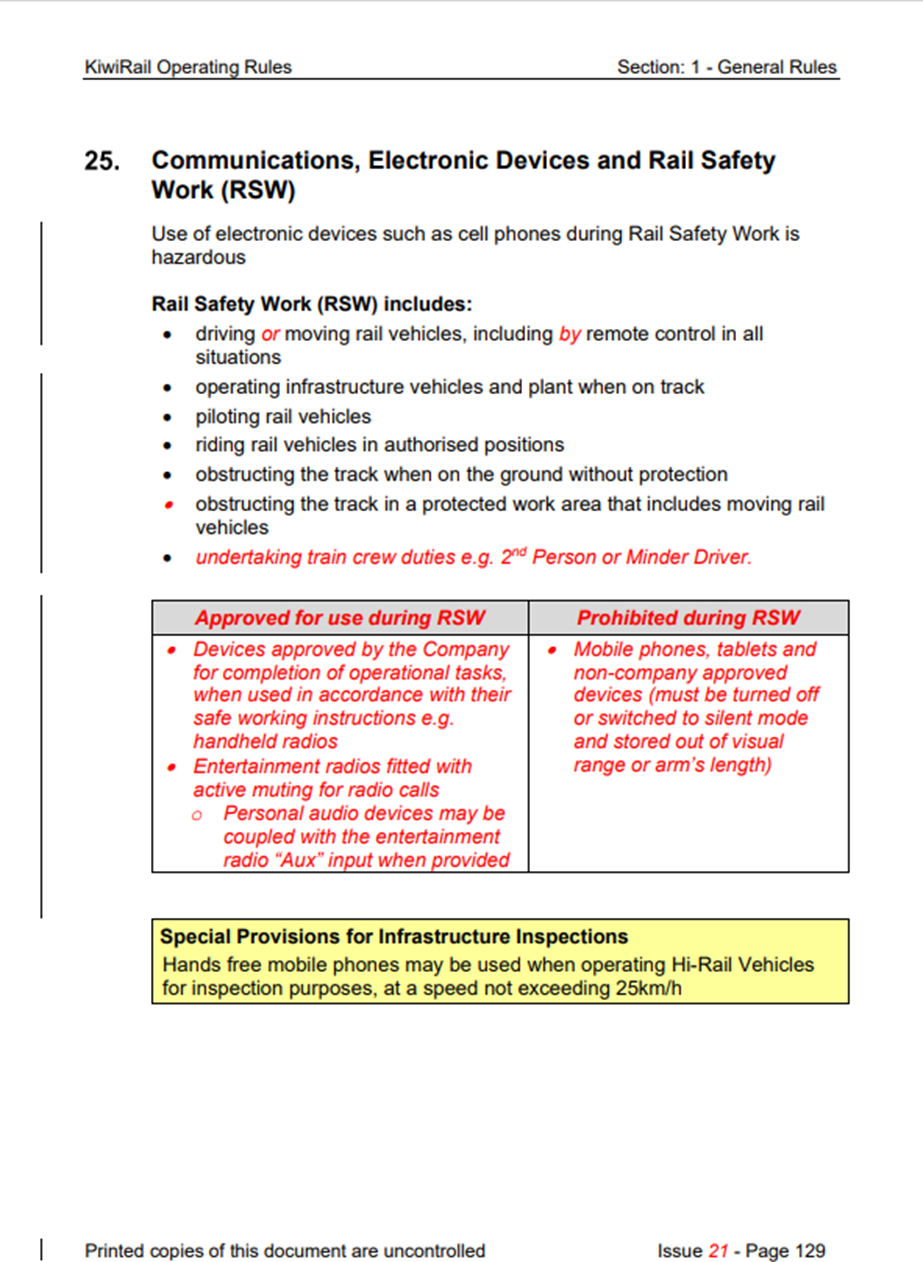
- KiwiRail’s Rail Operating Rules and Procedures, Section 1, Rule 25, prohibits the use of mobile phones, tablets and non-company-approved devices during rail safety work. This work includes driving and moving rail vehicles, including by remote control, in all situations (see Appendix 2).
Analysis Tātaritanga
Introduction
- Unintended rail movements in any situation are serious incidents with potentially serious consequences. On this occasion a shunt locomotive crossed an unprotected road crossing before entering the rail linkspan at Picton and entering Picton Harbour. Fortunately, the road crossing was not occupied at the time and there were no personnel working on the rail linkspan.
- The following section analyses the circumstances surrounding the incident to identify the likely cause of the incident and those factors that increased the likelihood of the event occurring or increased the severity of its outcome. It also examines any safety issues that have the potential to adversely affect future operations.
Why it happened
- The RCO had qualified only four months prior to the incident and could have been considered reasonably inexperienced. They had also taken three weeks’ leave during that four-month period.
- Due to disruptions in the rail ferry operating schedule, the day of the incident started off with shunting staff having a relatively low workload. However, as the shift progressed the workload increased, and it culminated in a very busy period – so much so that it resulted in the RCO having to carry out a series of tasks alone that they would normally have conducted as part of a two-person team.
- Acting on their own, the RCO made a mental plan of the tasks that needed to be completed during this time of increased activity, including advising the acting team leader that the refrigerated wagon was not located on Train 736 and that the movement of the head wagon to the CTT was taking longer than expected, and advising them of the action that needed to be taken to clear the fouled points and take the head wagon up to the CTT.
- It was at this time that the RCO removed their mobile phone from their pocket to contact the CTT, with the intention of advising the supervisor of the late arrival of the head wagon. However, aware that the regulations prohibited the use of mobile phones during operations, the RCO then decided not to continue with the call. The RCO then listened to a conversation occurring on the UHF radio.
- The RCO’s original task had been to manoeuvre the shunt locomotive clear of the fouled points to enable the points to be manually changed and the locomotive to move south towards west 6 road. However, the RCO moved on to the next task of walking south to meet the RO.
- The RO was at the south end of the yard, out of visual range of the RCO completing unrelated tasks (see Figure 6). The plan was for the RO to assist the RCO with the shunt movement from west 6 road to the CTT after completion of the RO’s tasks.
- While walking south towards west 6 road, the RCO turned their back on the shunt locomotive as it began moving north. The RCO did not complete the following tasks: checking that the shunt locomotive was clear of the points; stopping the shunt locomotive; moving 55 points manually; and changing the direction of the shunt locomotive to head south towards west 6 road. As a result, the shunt locomotive and the attached head wagon were able to proceed north, unintentionally in the direction of the rail linkspan.
- It is likely that during this period of increased work activity the RCO became distracted, continuing to operate the remote-control pack while walking south, away from the locomotive. The RCO’s attention was switching between multiple task demands in an effort to achieve all the required tasks efficiently prior to their shift handover.
- As the RCO worked at an increased pace, their attention switched to the next task prior to completing the task of clearing the fouled points and changing the locomotive direction to move south.
- As there was no feedback from the control pack to alert the RCO and aid error recognition, it was not until the RCO turned around to check the position of the shunt locomotive that they realised it had travelled in the opposite direction and was now on the rail linkspan.
- Although the RCO attempted a braking command on the remote control pack in the final seconds, they made no attempt to use the emergency brake. Even if they had done, it would very likely have been too late to prevent the shunt locomotive and attached head wagon entering Picton Harbour.
Shunting procedure and training
Safety issue: The RCO was working unaided when the incident occurred. Had the RO been present during the shunt procedure, it is very likely that the RCO would not have left the shunt locomotive and this incident would not have occurred.
- Shunting activity is relatively straightforward. However, the interaction of commercial timetables and scheduling priorities can result in periods of high workload.
- Prior to the incident, the RCO had been working alone at the north end of the yard, as the RO, who would normally have assisted the RCO, was carrying out other duties at the opposite end of the yard.
- Usually, the two would have worked together as a team within visual sight of each other. The RO would have been responsible for setting the route for any intended movements by manually operating points. The RCO would have remained with the shunt locomotive to control the movement.
- If they had worked together, the RCO might not have left the shunt locomotive and the RCO and RO would have been able to maintain visual contact. It is very likely that had the RCO and the RO been working together and in visual contact, this incident would not have occurred.
- KiwiRail advised the Commission that it was not normal practice for a shunt crew to work at opposite ends of a freight yard, out of visual range of each other. However, there was no rule or procedure stating that it was compulsory for them to work within visual range.
- The Commission has therefore made a recommendation in section 6 of this report to address this safety issue.
Safety issue: The process for supporting recently qualified staff in safety-critical roles was not managed effectively.
- Since being certified four months prior to the incident, the RCO had performed 48 shifts as a remote-control operator. The eight most recent shifts had taken place following a period of three weeks’ leave.
- At this stage of their development, the RCO should have undergone at least four assessments, known as safety observations, to assess their levels of competency, confidence and compliance with rules and regulations. According to KiwiRail’s Rail Operating Rules and Procedures, Section 10.3, the RCO should have been added to the support programme for new RCOs (see Appendices 1 and 2).
- The support programme had been developed to support recently certified staff to attain levels of competency that would assist them in achieving the required operating standards. In this case the programme should have started on 28 April 2021.
- Contrary to KiwiRail’s requirements, the recently certified RCO had not been added to the support programme upon certification, and the Commission found no evidence that these compliance checks had ever been performed.
- At the time of the RCO’s certification the KiwiRail Picton operations manager was aware that additional safety observations and coaching were required for the RCO as part of the support programme. However, the operations manager expected that the required frequency of these observations would be entered into the system by someone else when the mastery test documents were sent to the KiwiRail Learning Exchange (KLE).
- The manager was unaware that it was their responsibility to enter the initial certification and set monthly safety observations, as they had not received formal training in how to use KLE. KiwiRail advised that the use of KLE had not been included in the manager’s induction process.
- KiwiRail was also aware of an error with KLE, whereby the frequency of conducting safety observations of newly certified personnel d faulted to the standard eight-monthly cycle rather than monthly. To overcome this, managers were required to reset the safety observation frequency manually for anyone requiring these observations.
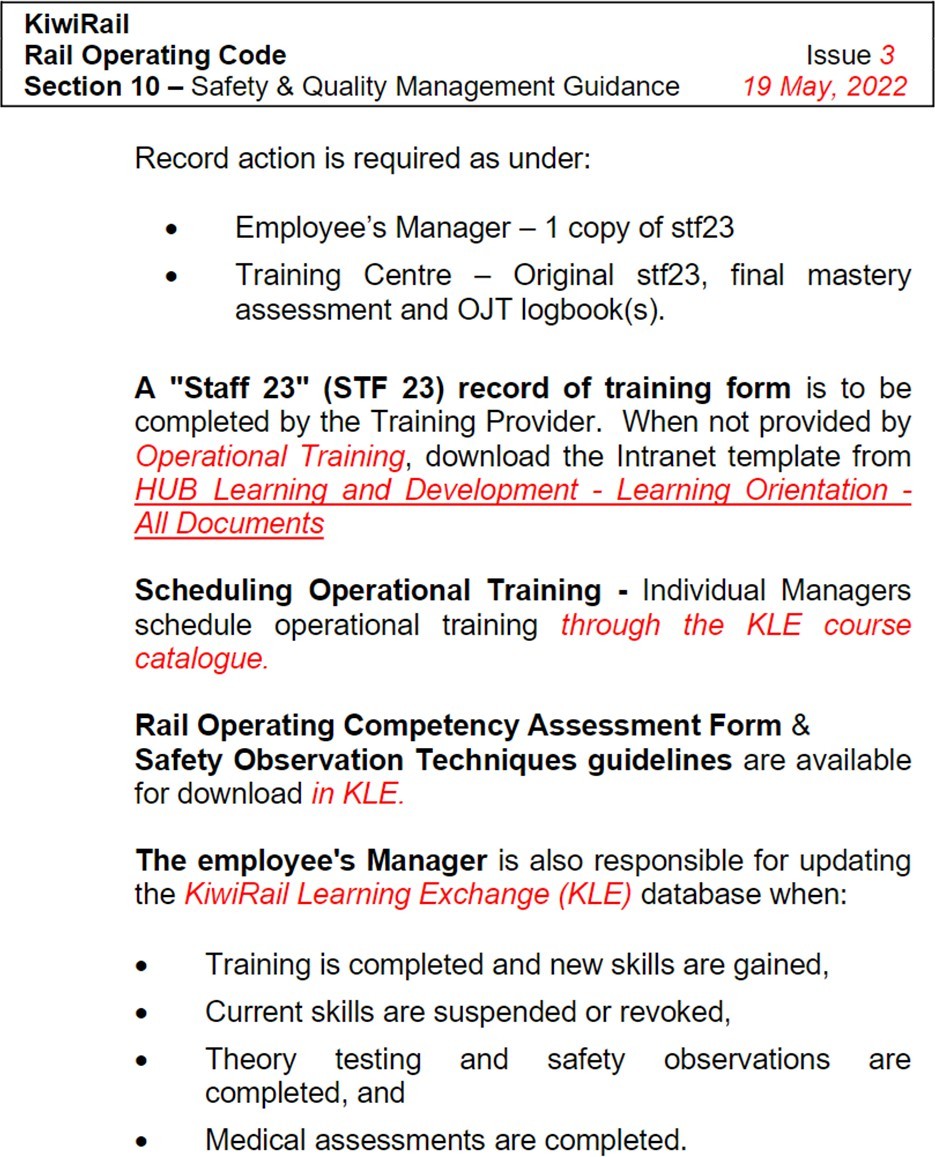
- The KiwiRail ROC, Section 10, Safety & Quality Management Guidance (see Appendix 3) made no mention of KLE, instead referring to the obsolete SMART database, which had previously been used to manage certification currency at KiwiRail.
- Had the RCO been added to the support programme and personnel received the scheduled regular assessments, any areas of concern may have been highlighted.
- While it was not considered to have contributed to this accident, the Commission found that KiwiRail’s support programme for newly trained operational staff was not managed effectively.
- That a safety-critical worker was not receiving support post-certification is of concern to the Commission. KiwiRail has since taken action to address this issue by updating its ROC, Section 10, Safety & Quality Management Guidance to reflect the actions necessary when utilising the KLE system (see Appendix 1).
- In the view of the Commission, this action addresses the safety issue, therefore no recommendation has been made.
Remote-control pack safety
Safety issue: The ROC contained little guidance on when remote-control units should be switched off and made safe to prevent unintended movements.
- The Commission found that at the time of the incident there was little guidance available as to when a remote-control pack should be turned off and made safe to prevent unplanned or unintended movements.
- The only reference to when the remote-control pack should be made safe to prevent unintended movements is in Section 5 of KiwiRail’s ROC on shunting procedures, which states ‘when carrying transition heads’, which was not a condition present during this incident.
- However, the RCO was very likely aware of the need to make the pack safe because earlier in the shift, prior to their taking a rest break, they had secured the locomotive by switching the remote-control pack off. This action applied the brakes and prevented any unintended or unplanned movements.
- The Commission found there was no clear guidance at the time of this incident on when the remote-control pack should have been made safe.
- On 17 March 2022 KiwiRail amended ROC Section 5.2 Remote Control Locomotive Procedures by issuing a Semi-permanent Bulletin No. 414 that described procedures for when remote-control packs should be made safe (switched off) to prevent unintended movements (see Appendix 4).
- In the view of the Commission this action addresses the safety issue, therefore no recommendation has been made.
Protection of the rail linkspan
Safety issue: There was no common understanding between KiwiRail and Port Marlborough on how to mitigate the risks to workers on or near the rail linkspan of unexpected rail movements.
- Port Marlborough was responsible for implementing a maintenance regime for the rail linkspan. At the time of the incident no maintenance was being carried out.
- The risk of rail movements entering the rail linkspan area when ferries were not in port had not been identified in KiwiRail’s ‘Picton operations site operation risk assessment’. Neither had the risk assessment considered the need to protect Port Marlborough staff working on and near the rail linkspan.
- The Commission found that there was no documented interoperability agreement between KiwiRail and Port Marlborough.
- On 7 April 2022, a Joint Operating Plan was signed between KiwiRail (licensed access provider and the sole shunter at the siding) and Port Marlborough (responsible for the maintenance of the linkspan).
- In the view of the Commission this action addresses the safety issue, therefore no recommendation has been made.
Safety issue: There was no physical protection in place to prevent unintended rail movements entering the rail linkspan.
- When facing the rail linkspan from west rail yard, a metal security gate can be seen. The purpose of this gate is to restrict the entry of unauthorised personnel to the rail linkspan. The security gate was open at the time of the incident, but it is not considered that it would have been effective in stopping the shunt locomotive accessing the rail linkspan and preventing this incident occurring.
- The Commission found that there were no engineering protections in place for the rail linkspan and any Port Marlborough staff who may have been in the vicinity of the linkspan at the time of the incident.
- Since the incident, a derailing block (see Figure 10) has been fitted to provide limited engineering protection against unintended movements entering the rail linkspan. Derailing blocks have limited effectiveness as they do not always work as intended and are reliant on rail personnel placing them in either the on or the off position.

- The Commission welcomes the actions taken to provide protection for the rail linkspan. However, further engineering control measures would provide an enhanced level of protection for workers, and therefore the Commission has made a recommendation in Section 6 of the report to address this safety issue.
Appendix 1. Updated Rail Operating Code
Appendix 2. Rail Operating Rule 25
Appendix 3. Training and Certification
Appendix 4. Semi-permanent Bulletin No. 414
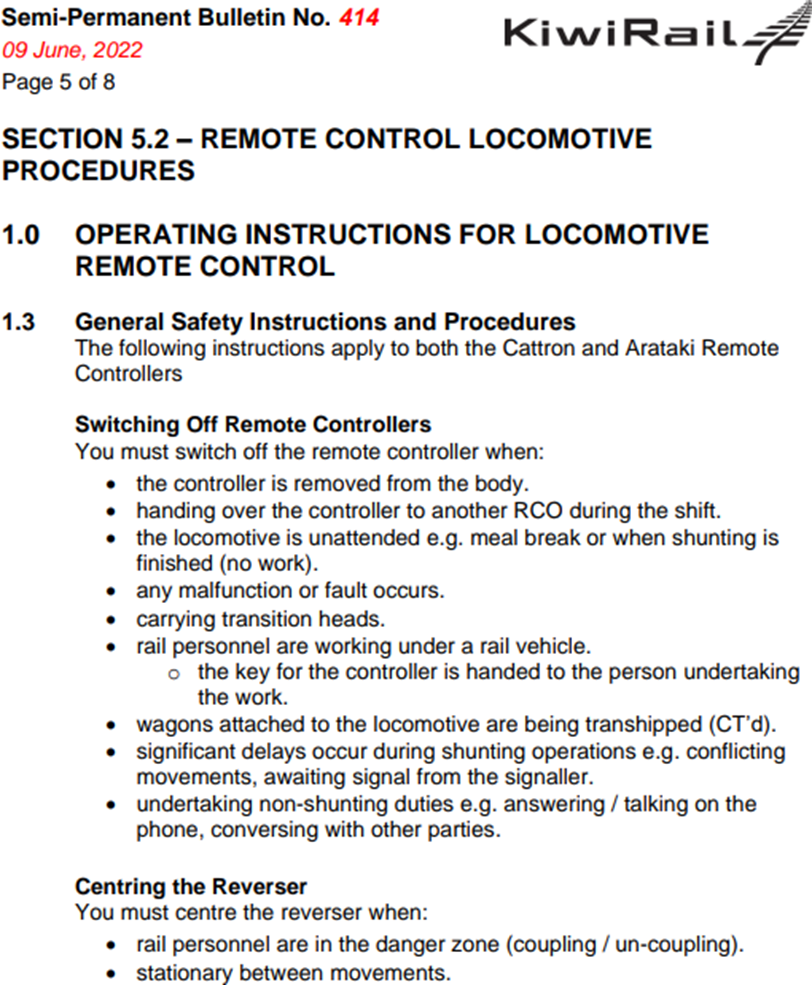
ROC Section 5.2 - Remote Control Locomotive Procedures