A helicopter accident occurred after maintenance work on a flight-control system. A critical securing bolt was not correctly installed and was not detected during duplicate inspections. Distraction, fatigue and weak assurance processes contributed to the error passing through maintenance checks before release to service.
Executive summary Tuhinga whakarāpopoto


What happened
- On 20 July 2024, a pilot and passenger were repositioning an Airbus Helicopter AS 350 BA helicopter, ZK-HJM (the helicopter) from Queenstown to Franz Josef after maintenance.
- After flying for about 52 minutes, the pilot felt a jolt in the airframe then noticed that the main rotor blade tips were no longer following the same path, as seen from the cockpit. About seven minutes later, when the pilot began a descent for a precautionary landing, the cyclic control (the control that changes the pitch angle of the rotor blades individually during a cycle of revolution, and as a result tilts the main rotor disc to control the direction and velocity of flight) became significantly harder to push in one direction. The helicopter was still controllable, and they continued to descend for a precautionary landing near a small settlement close to the Paringa River mouth.
- As the helicopter was approaching to land, at about 10 to 20 feet above the ground, it made an unintentional roll (the helicopter rolled about the longitudinal axis without conscious or deliberate control input from the pilot) to the left and then collided with terrain.
- The helicopter came to rest on its left side, facing about 180 degrees from the original direction of travel.
- The activation of the helicopter's emergency locator transmitter (an emergency locator transmitter transmits a distress signal to the Cospas-Sarsat search and rescue satellite system) alerted the Rescue Coordination Centre who dispatched a rescue helicopter to the site. Both occupants were transported to hospital with minor injuries. The helicopter suffered significant damage.
Why it happened
- The left and right main rotor hydraulic servo actuators (a servo is a hydraulic actuator that assists the movement of a mechanism) (the servos) were swapped over during the maintenance check prior to the accident flight. Both parts of the duplicate safety inspection (designed to verify that a critical maintenance task has been done correctly, and identify and capture any errors that may have occurred during the conduct of the maintenance task. It is not simply a process of confirming the work has been carried out, but a detailed review of the maintenance actions, see AC 43-1, 3.3) had been certified as complete by trained, qualified and authorised personnel.
- It is virtually certain that the bolt securing the lower end of the left-hand servo became detached during flight resulting in a change in the control characteristics of the helicopter and influencing the outcome of the landing.
- Despite the requirement for a duplicate safety inspection, and the number of pilot pre-flight inspections that were undertaken, it is very likely that the engineers who conducted each part of the duplicate safety inspection were distracted and did not adequately verify that the left and right main rotor servo swap had been completed correctly.
- It is likely that the engineer who certified the second part of the duplicate safety inspection was experiencing a level of cumulative fatigue (characterised by a progressive state of exhaustion that builds up over time due to consistent physical or mental exertion without sufficient recovery. Unlike acute fatigue, which can be resolved with a good night's sleep or a short break, cumulative fatigue persists and often requires more structured intervention to address. It is fundamentally a state of incomplete recovery from recurring stressors, leading to an increasing deficit in energy and performance over time) that contributed to the error.
What we can learn
- A thorough handover and pre-flight inspection are important following any maintenance activity, especially when there has been any disturbance of the primary flight controls.
- The duplicate safety inspection is an essential part of maintenance on critical flight controls and must be performed thoroughly and carefully.
- Proper and timely record keeping is an important part of the maintenance of aircraft and should be completed as soon as practicable at the completion of each task.
- Distractions, including interruptions, are an ever-present risk to aviation safety and need to be managed to ensure critical tasks are completed correctly.
- A run-on landing (a landing with significant forward motion, as opposed to a landing from a hover. After touchdown, forward motion is maintained until ground friction brings the helicopter to a halt. It is generally used when there is insufficient power to sustain a hover or to reduce the power required and control inputs required in some emergency situations where the integrity of the primary flight controls of a helicopter is unknown) with minimal changes to the flight controls and power required will usually provide the safest method to approach and landing when the integrity of the primary flight controls of a helicopter is unknown.
- On-board video recorders can provide valuable information for transport safety investigations to assist with determining the circumstances and causes of accidents and incidents, to avoid similar occurrences in the future.
Who may benefit
- All pilots, operators, maintenance providers and their staff may benefit from the findings in this report.
Factual information Pārongo pono
Narrative
Accident flight
- At 1347 on Saturday 20 July 2024, Airbus Helicopters AS 350 BA helicopter ZK-HJM (the helicopter), operated by Amuri Helicopters Limited (the operator), departed from the Salus Aviation (AW) Limited (the maintenance provider) hangar at Queenstown Aerodrome. It was a non-revenue repositioning flight to Franz Josef with two people on board.
- The helicopter had been released to service after completing planned maintenance, (see paragraph 2.16). The pilot had also flown the helicopter the previous day for a series of operational flight checks. The passenger (although there were two pilots on board, only a single set of flight controls were fitted for the right-hand pilot position) in their role as the operator’s chief pilot, had also flown the helicopter earlier in the day as part of the post-maintenance acceptance process.
- The accident flight was initially uneventful. The on-board video and audio recorder (on-board video) captured the pilot remarking how smoothly the helicopter was flying (recorded on the installed Eye In The SkyTM cockpit video recorder that also recorded intercom and radio communications) after the maintenance work (there had been several maintenance actions to improve the flight characteristics of the aircraft, including repairing the bracket for one of the vibration dampening weights under the floor of the helicopter, resetting the main rotor blade trim tabs to zero, then tracking and balancing the main rotor blades).
- About 52 minutes into the flight, the pilot reported feeling a slight jolt in the aircraft and commented to the passenger that the helicopter’s main rotor blades appeared to go ‘out of track’ (when the main rotor blade tips are not following the same path as seen from the cockpit). The pilot and passenger discussed the out-of-track condition and possible causes and initially chose to continue with the flight.
- About seven minutes later, after further discussion, the pilot and passenger collectively decided to make a precautionary landing to check the helicopter, near a settlement close to the Paringa River mouth.
- When the pilot lowered the collective to descend, the out-of-track and vertical vibration became more pronounced and they found that the cyclic control had become harder to move to the left. The pilot and passenger discussed the development, noting that it appeared to be consistent with a single hydraulic servo failure (a single hydraulic servo failure refers to a failure of a single component within a hydraulic servo system. This failure can be due to various reasons such as contamination, wear or inadequate maintenance. It is characterised by a specific malfunction of the servo valve, which can lead to reduced control precision).
- The pilot and passenger discussed the likelihood of a single hydraulic servo failure. The pilot informed the Commission that at the time they did not consider that they could have had either a main rotor servo slide valve seizure or a hydraulic system pressure loss. They then chose to land on a grass area near the Paringa River mouth. During interviews the pilot said that they intended to make a run-on landing to the flat grass area (see Figure 3).

- Immediately prior to landing, when the helicopter was about 10 to 20 feet above the ground, the on-board video showed the torque (the amount of torque is directly related to the amount of engine power being used to turn the main rotor disk, and the cockpit display is shown as a percentage of the maximum engine torque as defined by the manufacturer) increasing through 40 to 60%, and the pilot stated that they were ‘out of control’.
- The helicopter then commenced an uncommanded roll to the left, resulting in it impacting the ground and coming to rest on its left-hand side, facing about 180 degrees from the approach direction (see Figure 4).
- The passenger vacated the helicopter through the broken front left window. The pilot shut down the engine by closing the fuel lever, then also vacated via the same window.
- The helicopter’s emergency locator transmitter (ELT) was activated automatically on impact. The Rescue Coordination Centre (RCC) received an alert at 1451, and a search and rescue helicopter was dispatched.
- The pilot and passenger inspected the helicopter after the accident. They discovered a bolt missing from the lower attachment point where the left main rotor hydraulic servo connects to the transmission housing (see Figure 5 and Appendix 1). After the accident, the pilot and passenger located the bolt on the helicopter transmission deck. However, the nut was unable to be located at the site.
- The rescue helicopter arrived about 1600 and transported the pilot and passenger to Grey hospital in Greymouth with minor injuries.


- The maintenance records show that the left and right hydraulic servos had been swapped over during the maintenance activity prior to the accident. The swap was done at the request of the operator to balance wear on the components, and to improve the service life of the servo that is subject to higher workloads.
- Impact damage shows that during the accident sequence all four main transmission mounts failed in instantaneous overload. The right-hand hydraulic servo input rod broke in overload just above the transmission deck, and the right-hand cyclic bellcrank pivot bolt (the pivot bolt serves as the rotation point for the pivot arm. The bellcrank converts the control input into a different direction to actuate another component) sheared off at the thread end below the transmission deck.
Prior maintenance activities
- From 1 July to 20 July 2024, the helicopter underwent maintenance at the maintenance provider’s hangar at Queenstown Airport. This involved a 150-hour airframe and 300-hour engine check consisting of 67 scheduled (based on calendar and/or airframe hours) and 16 unscheduled (to rectify a defect or at the operator’s request) additional maintenance tasks. These tasks were published in a workpack (the repair, maintenance or overhaul instructions provided to the engineer for accomplishment of scheduled or unscheduled work. It can include work order/task cards) and made available to the engineers who would be working on the helicopter.
- The installation of the left hydraulic servo was certified as completed on 6 July 2024 in the workpack by Engineer A, who also certified the first part duplicate safety inspection for the same job on the same date.
- A duplicate safety inspection was certified as completed by Engineer B on Monday 15 July 2024.
- On Friday 19 July 2024, at the completion of maintenance, a foreign object debris/damage (any object found in an inappropriate location that, as a result of being in that location, can damage equipment or injure personnel) (FOD) check was completed prior to the helicopter being flown on a series of track and balance (rotor track and balance is a routine maintenance task that involves a calculated system of adjustments to pitch links, blade weights and trim tabs. These adjustments are designed to reduce vibrations at the fundamental (once-per-revolution) rotor frequency) flights, subject to the conditions of a limited release to service (refers to the formal declaration that the maintenance tasks on an aircraft (or component) have been carried out correctly by an appropriately authorised person, as per the requirements of CAR Part 43 Subpart C – Release to Service) (RTS) (for the purpose of operational flight checks). The flights were undertaken locally in the Queenstown area, and were to adjust the main rotor flight characteristics following maintenance activity. This included a pre-flight inspection by the pilot that conducted these maintenance flights, who was also the pilot on the accident flight.
- On the morning of Saturday 20 July 2024, Engineer B, who was the RTS Licenced Aircraft Maintenance Engineer (LAME), certified that the helicopter was in an airworthy condition following all maintenance activity.
- The chief pilot for the operator conducted a formal post-maintenance acceptance of the helicopter, including a pilot pre-flight inspection and an acceptance flight in the local area. The helicopter was then formally released to the operator.
- A minimum of four trained and qualified individuals inspected the helicopter for airworthiness prior to the accident flight. All were aware that during maintenance the left and right servos had been swapped over. They all had the opportunity to inspect the helicopter, and all certified that they had done so.
General Maintenance Rules
- The New Zealand Civil Aviation Rules (CARs) Part 43 General Maintenance Rules prescribes the requirements for the maintenance and RTS after maintenance of aircraft, and components to be fitted to aircraft, that are required by Part 91 (CAR Part 91, General Operating and Flight Rules) to have an airworthiness certificate issued under Part 21 (CAR Part 21, Certification of Products and Parts).
- Maintenance records must be completed in accordance with CAR 43.69. CAR 43.69(d) requires that a person performing maintenance on an aircraft or a component must, after recording the details required by paragraphs (a) to (c) of CAR 43.69, include the following information as part of the maintenance record:
- the person’s name
- the person’s signature except if the maintenance logbook or worksheet is in electronic format
- if applicable, the person’s licence, approval or authorisation number
- the date of the completion of the maintenance
-
Duplicate safety inspections are required for components of the flight control system (a system that has the ability to directly change the flight path, attitude, or propulsive force of an aircraft, and includes the flight controls, the engine and propeller controls, the related system controls, and the associated operating mechanisms: CAR Part 1, General Definitions) as they are critical to the safe operation of the aircraft (CAR Part 43.113). CAR Part 43.113 requires that no certification for RTS of aircraft/components is permitted after initial assembly, disturbance or adjustment of any control system part unless:
(a) the applicable requirements of Subpart C have been complied with; and
(b) a duplicate safety inspection has been carried out by an appropriately qualified person (as specified in CAR 43.113(b)(1)-(2)), to ensure that –
(i) the control system of the aircraft or the component functions correctly; and
(ii) in respect of the maintenance performed, the control system assembled correctly and every required locking mechanism is in place; and
(c) the certification and signatures required are complete.
-
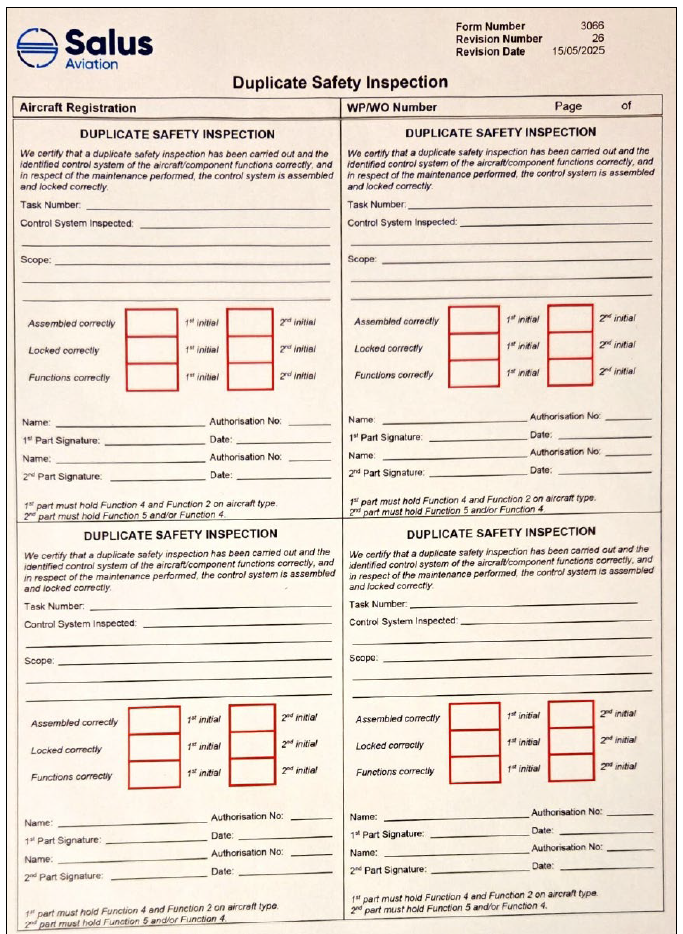
Following the completion of a duplication safety inspection, CAR 43.113(c)(3) prescribes the statement that must be entered in the appropriate maintenance logbook or worksheet by the person who carried out the inspection:
We certify that a duplicate safety inspection has been carried out and the identified control system of the aircraft/component functions correctly, and in respect of the maintenance performed, the control system is assembled and locked correctly.
-
CAR 43.113(d) outlines the details that must be entered in the maintenance logbook or worksheet adjacent to the statement required above, once the duplicate safety inspection has been carried out:
(1) the name of the person; and
(2) the signature of the person except if the maintenance logbook or worksheet is in electronic format; and
(3) the licence number, approval number, or authorisation number for the person; and
(4) the date of entry.
Personnel information
Pilot
- The pilot had been issued with a Commercial Pilot Licence (Helicopter) in November 1984, with the last renewal conducted in January 2023.
- The pilot’s last company check (a standard flight crew competency check was not required as the pilot performed CAR Part 91 General Operating and Flight Rules operations only and was not employed on a commercial basis) with the operator had been conducted in November 2021.
- At the time of the accident the pilot had a total flight time of 3981 hours, of which about 2857 had been on the AS350-type helicopter.
- The pilot was also a Licenced Aircraft Maintenance Engineer with 53 years’ experience. They had over 45 years’ experience on the AS350-type helicopter.
Passenger
- The passenger was the operator’s chief pilot and had been issued with a Commercial Pilot Licence (Helicopter) in July 2011.
- Their last company flight crew competency check with the operator had been conducted in August 2023.
- At the time of the accident the chief pilot had a total flight time of 5180 hours, of which 2500 had been on the AS350-type helicopter.
Maintenance personnel
Engineer A
- Engineer A was employed by the maintenance provider in June 2019. They initially joined as a trainee, and then in October 2021 they gained their aircraft engineer’s licence.
- Engineer A held several ratings, including a Group 2 rotorcraft rating. In November 2022 they were appointed as the maintenance provider’s Queenstown hangar foreman. Engineer A was authorised to release to service and to undertake first and second part duplicate safety inspections.
Engineer B
- Engineer B was employed by the maintenance provider in January 2019.
- Between January 2019 and November 2020, they were the helicopter maintenance manager for Queenstown. From November 2020 until the time of the accident, they had been working as the maintenance provider’s Queenstown chief engineer. Engineer B was a licensed aircraft engineer and held multiple ratings, including Group 2 for rotorcraft. Engineer B was authorised to release to service and to undertake first and second part duplicate safety inspections.
- They had over 45 years’ maintenance experience, mostly in the rotorcraft field.
Aircraft information
- ZK-HJM was manufactured as an Airbus AS 350 B helicopter, serial number 1671, constructed on 6 December 1982 by Eurocopter Helicopters in France under Type Certificate R008. The helicopter was converted to an AS 350 BA (FX2) in 2016, which included changing the single Safran Arriel 1B engine to the Honeywell International Inc LTS-101-700D-2 turboshaft engine.
- The helicopter had accrued 13,043.2 total flying hours since new at the time of the accident.
- A review of airworthiness was carried out on 28 December 2023, at 12,865.2 hours’ total time in service. The next review was due on 17 December 2024.
- Using the certified weight of the helicopter, and the weights and positions of the two occupants plus the calculated fuel load, the helicopter was calculated to be within its weight and balance limits at the time of the accident.
Recorded data
- The helicopter was fitted with a Tracplus™ RockAIR tracking system that recorded the helicopter’s flight path and provided a flight following and alerting service to the operator.
- The helicopter was also fitted with an Eye In The Sky™ on-board video and audio recording system. This recorded the flight path, speed, heading and altitude, as well as instantaneous acceleration in all three axes of movement.
Medical information
- Both the pilot and the passenger suffered minor injuries. The pilot was not wearing a helmet for this flight and was not required to do so. The passenger was wearing a helmet.
Tests and research
Hydraulic servos
-
As part of the investigation the three hydraulic servos were taken to an independent overhaul facility in Brisbane, Australia for expert evaluation under the supervision of a Commission investigator. The testing identified wear outside overhaul limits to the left main hydraulic (as it was at the time of the accident) servo. The report stated:
Servo-Actuators tested and evaluated using OEM CMM maintenance data 65-40-02 Rev 7 for P/N AC67246, and CMM 65-40-03 Rev 10 for P/N AC67244.
• Servo S/N CC426, piston speed in retract and extend was found to be outside of the CMM limits during the Speed Test. This is a result of both the Link Pin and Hinge Pins having wear outside the CMM limits.
• Internal leak in the retract position of the Servo Valve would be due to wear on the internal O-Rings.
Regarding the identified issues on S/N CC426 with operational speeds outside limits in both directions, the CMM test is conducted over a full piston cycle. When in service, the effect may appear negligible due to the occurrence of piston movements on a much smaller scale.
The report concluded that the effect of the wear may appear negligible when in service.
Fuel tank
-
The fuel tank ruptured during the accident sequence. At the request of the Commission, three-axis acceleration data and photos of the wreckage were passed to Airbus Helicopters through the French Bureau d'Enquêtes et d'Analyses (BEA). Airbus undertook a review of the evidence and advised that:
Given the impact conditions and structural deformations around the main fuel tank, it is not abnormal that it ruptured.
- Airbus further advised that crash-resistant fuel systems are available as retrofit solutions for the entire AS350/EC130 fleet. These solutions are proposed under the helicopter Type Certificate (TC) (A Type Certificate is issued by the National Aviation Authority (NAA) of the state of the operator, stating the airworthiness standard for the aircraft type, model, aircraft engine or aircraft propeller. The initial Type Certificate is likely to be obtained in the state of manufacture) or a Supplemental Type Certificate (STC) (an approval to carry out an aircraft type modification which is deemed by the Airworthiness Authority concerned to be a sufficient change to the original design of an aircraft type to require a specific validation).
Seats
- The pilot seat attachment point separated during the accident sequence, causing the seat and pilot to fall onto the floor-mounted control quadrant. This bent the collective control and prevented the pilot from being able to stop fuel flow to the engine immediately after the accident.
- The seats fitted to the helicopter were of the original design approved as part of the certification of the AS350 model helicopter. In 2000, the helicopter manufacturer offered owners the option to upgrade the installation of the current pilot and co-pilot bucket seats with a reinforced ‘standard’ seat attachment. Alternatively, the original seat could be replaced by a newer reinforced energy-absorbing design, and this was subsequently fitted to all new models of AS350/H125 helicopter from July 2008.
Organisational information
Salus Aviation (AW) Limited (the maintenance provider)
- The Queenstown maintenance facility was part of a nationwide maintenance and repair provider certified under CAR Part 145, Aircraft Maintenance Organisations. The maintenance provider's exposition described how maintenance was to be organised and conducted, and how that maintenance was to be recorded. A local maintenance manager was responsible for oversight of the maintenance facility. They were supported by a certifying engineer and a hangar foreman.
- The hangar foreman was responsible for managing resources and control of the workflow through the hangar. They would assign tasks to maintenance personnel and ensure that the standard of work met the organisation’s expectations. They would also ensure that the appropriate quality control checks were carried out during the maintenance work.
- The release to service engineer (certifies upon the completion of any maintenance carried out on an aircraft and its components that the ordered maintenance has been properly carried out in accordance with appropriate organisational procedures and regulatory requirements) was responsible for ensuring that aircraft left the hangar in an airworthy condition and that all associated documentation for its return to service had been completed. They were expected to personally inspect each aircraft to ensure that maintenance had been completed in conformance with technical data.
- Maintenance engineers were responsible for performing allocated maintenance tasks within the scope of their company authorisations. They were to advise the certifying engineer if any control system had been disturbed so that the certifying engineer could initiate a duplicate safety inspection.
- All staff were expected to be alert to safety hazards and raise a safety report if they identified a hazard.
-
The organisation’s Safety Management System referenced the use of Standard Practice Instructions (SPI) including SPI105 – Workpack Compilation, Completion and Certification, which included the following instructions.
Progressive Detailing and Signing
All preformatted maintenance schedule worksheets must be signed as the tasks are completed. The following information shall be included when completing and recording tasks:
- Date task carried out.
- Certifying Engineer second inspection check and signature.
- Referenced receiver numbers (batch numbers) for standard parts and consumables, not already recorded within the MRO IT system against a scheduled or unscheduled maintenance task.
- Calibrated tooling used referencing tooling number and measurement (if required).
- Referencing when a Duplicate Safety Inspection or stage inspection is required.
- Authorised Release Certificate or Form One information as applicable.
- Signing the AME and Rated LAME column, this confirms that the information provided on the worksheet has been referenced appropriately and associated tasks have been carried out.
- If a maintenance task cannot be completed in its entirety, then the engineer must raise a work entry into the appropriate aircraft worksheet for the stage at which the relevant task is complete. A subsequent work entry shall be raised for the remaining steps that must be completed to complete the task in full and a verbal handover is to take place between the engineer carrying out the task and the release to service or certifying engineer as applicable.
-
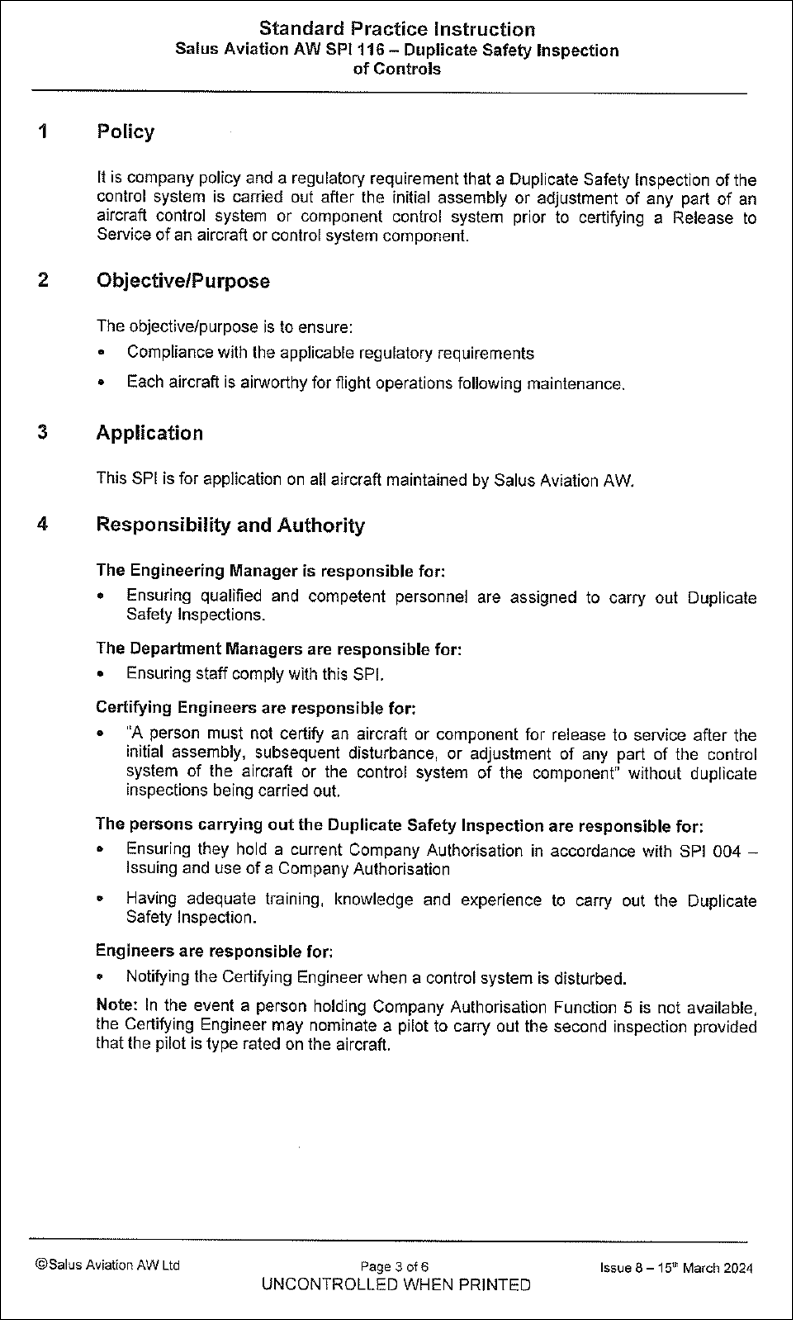
SPI116 Duplicate Safety Inspection of Controls (see Appendix 2) also included the following instructions for duplicate safety inspections.
Carrying Out the First Part Duplicate Safety Inspection
This person shall ensure that:
1. They are appropriately rated and authorised to carry out the first part duplicate inspection
2. Current Technical Data was used for the work
3. All parts of the system which have been disturbed are free from defects;
including:- Incorrect rigging
- Incorrect locking
- Any possibility of fouling or jamming
-
For the complete system, the controls function throughout their range of travel in each mode, and with each alternative means of actuation;
i. Freely and in the correct sense
ii. Without excessive backlash
iii. With the correct static friction
Carrying Out the Second Part Duplicate Safety Inspection
This person shall ensure that:
1. That they are appropriately authorised to carry out a Second Part Duplicate Inspection
2. Current Technical Data was used for the work
3. All parts of the system which have been disturbed are free from defects;
including:- Incorrect rigging
- Incorrect locking
- Any possibility of fouling or jamming
-
For the complete system, the controls function throughout their range of travel in each mode, and with each alternative means of actuation;
i. Freely and in the correct sense
ii. Without excessive backlash
iii. With the correct static friction
Amuri Helicopters Limited (the operator)
- Amuri Helicopters Limited was based at Hamner Springs. It had a fleet of three helicopters, comprised of two Airbus AS350 FX2s and one MD Helicopters MD520N. It operated nationwide to include a wide range of commercial operations.
Other occurrences
- The Commission identified previous occurrences that involved the lower attachment point of a main rotor hydraulic servo becoming disconnected during flight.
- One such occurrence (Airbus Helicopters Alert Service Bulletin (ASB) 67-00-77 (AS 350 B3)) involved an AS365 N3 Dauphin helicopter, which the BEA reported was being operated by the French Military. Airbus Helicopters treated it as a major incident and produced an Emergency Alert Service Bulletin on 25 July 2019 (which was updated on 03 February 2025) that described the failure as a result of incorrect maintenance actions.
-
Another occurrence involving an AS 350 BA, where the left lateral flight control servo became disconnected in-flight at the transmission, occurred in Princeville, Hawaii, USA in March 2007 (National Transport Safety Board, 2009). This accident was investigated by the United States of America National Transportation Safety Board (NTSB). The NTSB determined the probable cause(s) to be:
The failure of maintenance personnel to properly tighten (torque) the flight control servo lower attachment clevis, and reinstall a functioning lock washer, which resulted in a flight control disconnect and a complete loss of helicopter control. Contributing to the accident was the operator's failure to ensure its maintenance program was being executed in accordance with Federal regulations.
-
The Commission also identified other instances where the duplicate safety inspection process had failed to capture incomplete or inaccurate maintenance activities. The Civil Aviation Authority of New Zealand (CAA) published an educational article titled The life-saving importance of the duplicate inspection in the Autumn 2025 issue of Vector. The article stated that there were four (including this accident) known instances in the second half of 2024 where ineffective duplicate safety inspections were carried out. It reported that:
In all cases it was not an instance of the duplicate inspections not being done – they all were. It’s that the inspection failed to identify issues in one or more of the critical elements required to be checked during the duplicate inspection.
- The article referenced an earlier article published in the Winter 2022 issue of Vector that highlighted the importance of the duplicate safety inspection process (https://www.aviation.govt.nz/assets/publications/vector/vector-2022-2-winter-web.pdf), reinforcing that this is a known and ongoing issue in the aviation industry.
- On 19 February 2026, the maintenance provider notified the Commission of a related maintenance incident. On 12 January 2026, two engineers were tasked with connecting dual-control tail rotor pedals on two helicopters. The duplicate safety inspections that were carried out on both helicopters did not identify that ‘lock-out position’ pins had not been installed in accordance with the relevant maintenance instruction, and the helicopters were not in an airworthy condition when released to service. The fault was detected during a pilot pre-flight inspection of one of the helicopters the next day.
- The maintenance provider's internal investigation identified further safety improvements that the maintenance provider was in the process of implementing (see paragraph 5.3).
- TAIC inquiry AO-2001-009: Bell 206 ZK-HWI, engine power loss after take-off, Mount Pisa station Lowburn, 12 August 2001. The Commission identified a safety issue with the need for the helicopter maintenance company, in conjunction with operators it provides services for, to establish a robust system that ensured any additional maintenance is recorded correctly, so additional maintenance is completed fully at the earliest opportunity.
- The Commission recommended to Airwork NZ to establish a system, in conjunction with any operators for whom Airwork NZ provide maintenance services, that ensures any follow-up maintenance action necessary after any maintenance is correctly recorded and carried out at the appropriate time (013/02).
- TAIC inquiry AO-2002-003: Schweizer 269C helicopter, ZK-HIC, loss of tail rotor authority and emergency landing, Karaka Downs South Auckland, 15 March 2002. The Commission identified a safety issue with the need for duplicate inspections of helicopter tail rotor drive trains.
- The Commission recommended to the CAA to critically examine the requirements for duplicate inspections of aircraft control systems, with a view to including helicopter tail rotor drive trains as part of the duplicate inspection regime (037/02).
- TAIC inquiry AO-2005-007: Piper PA34-200T Seneca II, ZK-MSL, Wheels-up landing, Napier Aerodrome, 7 July 2005. The nose gear had failed to extend because the centring spring attachment bolt had jammed against the nose gear door aft tube assembly. The bolt had been installed incorrectly nine weeks earlier during maintenance. Safety issues identified by the Commission included the need for aircraft maintenance engineers to refer to appropriate documentation when carrying out unfamiliar tasks, the ongoing compliance with an Airworthiness Directive concerning the attachment bolt, and the effectiveness of the associated Service Bulletin.
- Safety recommendations were made to CAA and to the aircraft manufacturer regarding the Airworthiness Directive and Service Bulletin respectively (076/05) (104/05). The maintenance provider took action to improve staff maintenance practices, therefore no safety recommendation was made to that organisation.
- TAIC inquiry AO-2011-004: Piper PA31-350 Navajo Chieftain, ZK-MYS, landing without nose landing gear extended, Nelson Aerodrome, 11 May 2011. The safety issue identified by the Commission was an inadequate standard of maintenance performed by a range of organisations and persons on the aeroplane, and the standard of maintenance for general aviation aircraft in New Zealand needed to be improved.
-
The Commission made two recommendations to the CAA.
1. That they widen the range of aircraft systems that require duplicate checks after specified maintenance, at least for those aircraft used in air transport operations, in order to reduce the likelihood of recurring defects and incidents (019/13).
The Director of Civil Aviation replied:
The CAA considers that widening the scope of aircraft systems requiring duplicate inspections [is] not sufficiently supported by the Commission’s investigation. In this regard, the CAA prefers to remain in keeping with current world regulatory practice and therefore will not implement the recommendation.
2. That they take action, in concert with the aviation industry, to improve the level of compliance with Civil Aviation Rules and conformance with industry best practice throughout the general aviation maintenance sector (018/13).
The Director of Civil Aviation replied:
The CAA will not implement the recommendation as worded. However, the CAA will adopt the safety surveillance practices as described in our final draft report response letter 14 June 2013.
The relevant portion of the CAA letter of 14 June 2013 stated:
The CAA considers a recommendation that would address the relationship issues in terms of communications and record keeping between CAA Rule Part 43 maintenance providers and Part 135 AOC holders would be more effective. To this end, the CAA intends to profile Part 43 maintenance providers in order to identify poor performance or other risk issues. It is envisaged that increased surveillance and education programs would follow.
- Australian Transport Safety Bureau (ATSB) AO-2017-078: Loss of cyclic control and in-flight break-up involving Robinson R22, VH-HGU, 7 km north-north-west of Cloncurry Airport, Queensland, on 2 August 2017. The safety issue identified by the ATSB was that Cloncurry Air Maintenance had adopted a number of practices, which included using abbreviated inspection checklists, not recording all flight control disturbances and not progressively certifying for every inspection item as the work was completed, which increased the risk of memory-related errors and the omission of tasks.
- The Australian Civil Aviation Safety Authority issued Airworthiness Bulletin 67-005: Robinson Helicopter Flight Controls – Independent Inspections. The bulletin highlighted the need for independent inspections to be conducted and ‘recorded consecutively with each adjustment made during rotor tracking and balancing’ activities. The bulletin also identified several human-factor elements that could impact maintenance inspection performance, and highlighted the need for extra caution to be exercised during post-maintenance flights as per the guidance provided by Robinson.
- Transportation Safety Board of Canada (TSB): Loss of control and collision with terrain Diamond Aircraft Sales USA Inc. Diamond Aircraft Industries GmbH DA 42 NG, N591ER London Airport, Ontario, 25 May 2022. TSB made the following findings as to risk.
- If maintenance personnel are not trained on company procedures and applicable regulatory requirements before being authorized to perform or certify maintenance, there is a risk that the aircraft will not be airworthy when it is returned to service.
- If procedures requiring the inspection of flight controls do not provide specific instructions regarding how to ensure the surface is moving in the correct direction, flight controls that have been rigged in reverse may not be recognized.
- If the person signing a maintenance release for work accomplished by another person does not observe the work to the extent necessary to ensure that it is performed in accordance with the applicable standards of airworthiness, there is a risk that the aircraft will not be airworthy when it is returned to service.
Summary
- The Commission notes from the domestic occurrences there has been a pattern of maintenance errors, not captured by the duplicate safety inspection process, that have resulted in incidents and accidents. Recommendations consistently call for robust, mandatory double-checks for safety-critical work, improved maintenance record keeping and formal tracking of deferred actions to stop critical tasks being missed. The Commission has identified a related safety issue that is discussed further from paragraph 3.20.
- The Commission identified the following themes in international occurrences.
- True independence/methodical dual inspection is essential – a second signature is not enough.
- Functional verification must supplement paperwork checks.
- Human factors (fatigue, rushed work, unclear roles and divided responsibilities) often defeat the intent of duplicate inspections.
- International recommendations focused on making duplicate safety inspections mandatory for critical systems, including functional checks, documenting in detail and supplementing with training on human error/human factors.
Analysis Tātaritanga
Introduction
- The pilot lost control of the helicopter in the final stages of a precautionary landing, after noticing a change in the flight characteristics of the helicopter while flying straight and level on a repositioning flight.
- The accident occurred after the helicopter had been released to service following maintenance, which included disturbing the primary flight controls. A bolt that was meant to be securing one of the critical flight controls was discovered to be missing from its correct location after the accident.
- The following section analyses the circumstances surrounding the event to identify the factors that increased the likelihood of the event occurring or increased the severity of its outcome.
What happened
In-flight abnormalities and emergencies
- The pilot reported feeling a slight jolt in the aircraft and then immediately noticed that the helicopter main rotor blades had started flying out of track about 52 minutes into the flight.
- When the pilot lowered the collective to descend for a precautionary landing, about seven minutes after noting the blades going out of track, they found that the cyclic control became hard to move to the left. The pilot and passenger discussed these symptoms, including that it appeared to be consistent with a single hydraulic servo failure.
- During interview, the pilot stated that they elected to keep the hydraulics on as they believed they did not have a total hydraulic failure, but possibly a single hydraulic servo failure. This was because the control response was not as severe as a hydraulics failure (based on previous experience of turning off the hydraulics system during testing) and there was no HYD (the hydraulic system warning light is labelled as HYD on the helicopter annunciator panel) warning light or horn. They stated that they did not want to make the situation worse by turning off the hydraulics.
- The on-board video footage showed that the pilot made a shallow approach to land on a clear area that appeared suitable for a no-hover/slow run-on landing.
- The footage also showed that during descent the torque was low, from 10 to 30%. However, on short finals the torque increased through 40 to 60% and the pilot stated they were out of control immediately before the helicopter rolled left and impacted the ground.
- The bolt that connected the lower ball end fitting of the rotor actuator to the main gear box (MGB) was found on the transmission deck of the helicopter after the flight. It is very likely that the actuator bolt’s movement from one side, where the lower ball end fitting connects to the MGB conical housing (the MGB conical housing is the cone-shaped enclosure containing the helicopter’s main gearbox), manifested through the main rotor controls as a slight jolt in the aircraft and then the initial out-of-track condition. As the bolt was still part-way through the connection, hydraulic assistance from the left servo was still being provided.
- When the pilot lowered the collective to descend to the river for a precautionary landing, the torque reduced, which decreased the load through the main rotor control system. It is very likely that this allowed the loose bolt to fall completely free, thereby disconnecting the lower end of the hydraulic servo from the MGB conical housing.
- Once disconnected, the hydraulic servo was still working normally. However, the lower end had nothing to push against to provide hydraulic assistance to the pilot on that control (see Figure 6).
- The control rod that linked the pilot’s controls to the main rotor was still connected to the non-rotating swashplate via the upper end of the hydraulic servo.
- The flight manual stated that the AS350 helicopter was controllable with inoperative hydraulics, however the load feedback can be very heavy, especially at higher airspeeds. When a single hydraulic servo is no longer providing assistance on one of the three controls, in this case due to the disconnection of the lower attachment point from the MGB conical housing, the pilot is subject to those loads in one direction. This condition would exhibit symptoms as a heavy cyclic on one side.
- When the collective is raised in this situation, all three control rods are raised; however only two are hydraulically assisted, while the third is not. This will manifest as the cyclic pushing towards the unassisted side and requires the pilot to be able to match the force exerted by the hydraulic system on the still-connected servos.

- The pilot intended to make a run-on landing with minimal power changes close to the ground. The helicopter began rolling to the left following an increase in torque at about the point the collective would usually be raised to counter the loss of translational lift (translational lift refers to the increased efficiency of a helicopter's rotor system as it transitions from a hover to forward flight, resulting in improved lift and performance) during a normal approach (a normal approach and landing involves an approach to a hover, then vertical descent to skid touchdown).
- It is virtually certain that the increase in torque was due to the pilot raising the collective in response to a combination of the helicopter slowing and losing translational lift.
- It is very likely that due to the lower end of the hydraulic servo not being attached, and the hydraulic system being active during the precautionary landing, there was an overwhelming load on the unassisted control. This led to the helicopter making an unintentional roll to the left as the collective was raised on short final.
- A bolt securing the lower attachment point where the left main rotor hydraulic servo connects to the transmission housing was discovered to be missing after the accident. The bolt was found on the transmission deck; the nut was not found.
- It is virtually certain that the bolt securing the lower end of the left-hand hydraulic servo became detached during flight, resulting in a change in the control characteristics of the helicopter and influencing the outcome of the landing.
Quality assurance of maintenance activity
Safety issue: The maintenance provider did not have a robust quality assurance process to ensure maintenance activities were being completed and documented in accordance with their approved maintenance procedures. This increased the risk of maintenance errors not being identified and rectified.
Installation of the main rotor hydraulic servos
- The helicopter was flown to the maintenance provider’s facility in Queenstown on 30 June 2024. From 1 July to 20 July 2024, the helicopter underwent maintenance.
- The LAMEs involved stated during interviews that the operator made it clear to the maintenance provider that there was no time pressure for the release of the helicopter back into service.
- The maintenance on the helicopter involved a 150-hour airframe and 300-hour engine check consisting of 67 scheduled and 16 unscheduled additional maintenance tasks. These tasks were published in a workpack and made available to the engineers who would be working on the helicopter. Engineer A initially took responsibility as the release to service engineer,9F meaning they would assume responsibility for oversight of the work being done on the helicopter.
- Part of the unscheduled additional maintenance tasks that the operator had requested was to swap the left and right main rotor control hydraulic servos with each other. As this involved disturbance of the flight controls, a duplicate safety inspection was required following the completion of the task
- On the morning of 6 July 2024, Engineer A (who was not rostered to be working that day) arrived at the hangar to carry out some maintenance on their personal road vehicle. Two other engineers who were rostered on were at the hangar, working on another aircraft.
- After approximately four hours, Engineer A packed up their tools and was preparing to go home when they decided to paint the helicopter’s main rotor mast. Engineer A reasoned that if they did that task while they were at the hangar, the paint would be dry for their next rostered workday, 8 July 2024.
- At the completion of painting, Engineer A decided to do some additional work on the helicopter (at this point they booked themselves onto the company system to officially record their work hours). This included:
- reinstalling the hydraulic tank
- swapping the left and right main rotor hydraulic servos
- cleaning the tail rotor gearbox sight glass
- charging the hydraulic accumulators with nitrogen.
- Engineer A used a sonic cleaning bath to clean the sight glass. This involved periodically leaving the helicopter, where they were fitting the servos, to check how that task was progressing. Following installation of the right servo (this was the servo that had previously been on the left-hand side of the helicopter prior to the swap). Engineer A continued with the same task on the left-hand side. While they were working, a customer approached the hangar which interrupted Engineer A’s work for about 10 minutes.
- When Engineer A returned to the helicopter, they noticed that hydraulic fluid was dripping from two of the hydraulic hoses that had yet to be connected. They cleaned up the fluid spillage and set about connecting the two hoses. Engineer A later recalled that sorting out the leak had taken ‘quite a while’.
- The last task Engineer A worked on that day was charging the hydraulic accumulators with nitrogen. They then packed up and left the hangar at around 1600. Many of the tasks that Engineer A performed that day were disrupted, either by having to shift focus between different maintenance activities or by unplanned interruptions.
- On 9 July 2024, Engineer A took a photograph of another part of the hydraulic system, which also happened to show the lower attachment bolt on the left hydraulic servo with the nut only partially done up (see Figure 8 (this photograph was taken on 9 July 2024 and shows the state of the bolt and nut at that time)). There is no evidence of work being done on the left-hand hydraulic servo between the time the photo in Figure 8 was taken on 9 July 2024 and the helicopter departing on the accident flight.
- On Friday 12 July 2024, Engineer A completed the paperwork that related to the maintenance activity they had undertaken on the helicopter the previous weekend. This was inconsistent with CAR 43.69(d) which required that on completion of the maintenance, a person performing maintenance on an aircraft or a component must include the date of completion of the maintenance as part of the maintenance record.
- Additionally, the maintenance provider’s procedures (SPI105) required that the maintenance schedule worksheets be signed as the tasks are completed; and if a maintenance task cannot be completed in its entirety, then the engineer must raise a work entry into the appropriate aircraft worksheet for the stage at which the relevant task is complete (see 2.57).
-
Advisory Circular (AC) 43-1, 2.16 provides guidance on CAR 43.69(b) (CAR 43.69 (b) A person performing maintenance on an aircraft or a component may use associated worksheets to record the details of the maintenance performed if (1) a summary of maintenance performed is recorded in the appropriate maintenance logbook; and (2) the worksheets are referenced in the summary of maintenance required under paragraph (b)(1)) and emphasises that worksheets should be kept up to date during maintenance. It states:
Worksheets provide the operator and maintenance provider with a valuable record of maintenance undertaken. They should be compiled in a way that is easily understandable for anyone not associated with the maintenance task.
Worksheets should be kept up to date during maintenance so that they accurately reflect the aircraft status. Various accidents have been attributed to incomplete maintenance where maintenance providers have initiated a maintenance action without making a record in an appropriate document. Accurate work records assist the certifying engineer in ensuring that all necessary maintenance, including work arising during the check, is complete and that the aircraft is in an airworthy condition prior to release to service. They also support the operator in making an assessment that all necessary maintenance has been completed prior to returning the aircraft to operation.
…
All worksheets and associated documentation should be complete prior to the certifying engineer issuing the release to service.
- During inspection of the helicopter, Commission investigators found the upper attachment on the same hydraulic servo had the bolt in place with the nut attached to the bolt (see Figure 8). However, the nut was not tightened fully and did not have a locking pin installed. This was not in accordance with the manufacturer’s instructions, which required the nut to be tightened to a specific torque and then secured with a locking pin.
- It is virtually certain the nut was not tightened to the correct torque, and the locking pin that was meant to prevent the nut from coming loose was not installed, or not installed correctly, prior to the helicopter’s departure from Queenstown.
- Engineer A informed Commission investigators that while they had some memory of working on the right-side servo, they could not recall any details about work on the left-side servo. It is virtually certain that Engineer A did not complete the task of installing the left hydraulic servo.


First stage of the duplicate safety inspection and handover to the return to service engineer
- Engineer A returned to work on 8 July 2024. Due to a change in priorities from the operator, they spent the following four days working on the operator’s MD 500 while another engineer, Engineer B, conducted repair work on the helicopter.
- Following the MD 500’s release to service on 11 July 2024, Engineer A focused on preparing to hand over the responsibility as the helicopter RTS engineer to Engineer B. This was necessary as Engineer A was going on holiday and would not be available to release the helicopter to service at the planned completion of work.
- Engineer A recalled spending the afternoon of 12 July 2024 completing paperwork for the helicopter. This included ensuring that all the task items scheduled for the helicopter were showing in the workplan that had been generated for the engineers. As some items were not showing, Engineer A added them manually and marked off what had been completed and what work remained.
- Engineer A dated their certifying signature for the first part of the duplicate safety inspection for the items completed earlier in the week to match when they thought the inspection was completed, rather than the date the paperwork was completed (CAR 43.113(d) requires the date of entry to be included in the appropriate maintenance logbook or worksheet adjacent to the statement required by CAR 43.113(c)(3)).
- The handover briefing was conducted on Friday 12 July 2024, at a computer station adjacent to where the helicopter was positioned in the hangar. During Commission interviews, both engineers stated that they did not physically inspect the helicopter at any stage of the briefing. Engineer B recalled that the handover briefing took place at the end of the workday and lasted around 20 to 30 minutes. Engineer B recalled leaving for the weekend immediately after the briefing, at around 1700.
- As a critical flight control component, a duplicate safety inspection of the servo installation was required. During the handover, Engineer A advised Engineer B that they would have to do the second part of the duplicate safety inspection. Duplicate safety inspections were required for certain tasks, including the removal and reinstallation of the hydraulic servos, which were classified as critical flight controls due to their potential to adversely affect the controllability of the helicopter if not installed correctly.
-
As a qualified LAME, Engineer A was authorised to sign off on the first part of the duplicate safety inspection for the installation of the servos, in accordance with CAR Part 43.113(c)(3):
We certify that a duplicate safety inspection has been carried out and the identified control system of the aircraft/component functions correctly, and in respect of the maintenance performed, the control system is assembled and locked correctly.
- It is very likely that Engineer A was distracted in their work and under time pressure as they were going on leave, and that they did not adequately verify the left and right main rotor servo swap had been completed correctly at the time they signed the first part of the duplicate safety inspection certificate.
Second stage of the duplicate safety inspection and release to service
- Engineer B returned to work on Monday 15 July 2024. The pilot (the pilot was also a LAME employed by the maintenance organisation on a casual employment basis) who was going to fly the helicopter following its release to service later in the week, was at the hangar to undertake some maintenance work for the maintenance provider. Engineer B briefed the pilot on how the maintenance was progressing before the pilot began working on another aircraft.
- Engineer B then refamiliarised themselves with the helicopter’s workpack. Up until that point of the maintenance check, they had been engaged in repair under the helicopter’s fuselage. Once they had reviewed the workpack, Engineer B elected to conduct the second part of the duplicate safety inspection that had been discussed with Engineer A during the handover briefing. This included the inspection of the left and right main rotor hydraulic servos that Engineer A had swapped.
- During interview, Engineer B stated that they remembered inspecting the servo on the right-hand side of the helicopter. They also recalled looking through to the left-side servo but, as they could not inspect all the necessary components from their viewing position, they were aware that they would have to move to the left side of the helicopter to complete the inspection. However, they did not have any distinct memories of inspecting the left servo.
- During their shift on Monday 15 July 2024, Engineer B undertook several duplicate safety inspections on the helicopter, including signing for the second part of the duplicate safety inspection for the left and right hydraulic servo swap. In doing so they were certifying that they had checked that the identified control system functioned correctly and, in respect of the maintenance performed, the control system was assembled and locked correctly.
- On Tuesday 16 July 2024, Engineer B undertook work to connect the left and right hydraulic servo input rods. These had deliberately been left undone by Engineer A to facilitate the underfloor connection to the flight controls, and they communicated this to Engineer B during the handover. The position of the left input rod is in close proximity to the lower left servo connection (see Figure 9). However Engineer B noticed nothing untoward while they were connecting the input rod.
- Another opportunity arose to notice the incorrectly installed servo on Thursday 18 July 2024. Engineer B tasked the pilot with carrying out the second part of the duplicate safety inspection for the connection of the hydraulic servo input rods they had completed two days earlier. During Commission interviews, the pilot recalled that despite the input rod connection being in close proximity to the lower hydraulic servo connection, they were focused on inspecting the input rods and noticed nothing untoward.

Human error in maintenance
- Humans are known to make errors (slips, lapses or mistakes) when working, which is why sociotechnical systems (relates to an interconnectedness between humans and technology within a system. Complex systems have multiple individual, but inter-related, components that interact. Within complex systems, safety is considered to be an emergent property of the system as a whole, not the result of individual components acting in isolation) must be designed to be resilient to any human errors that occur.
- The aviation maintenance system requires a duplicate safety inspection of any flight-critical systems. A flight-critical system is any system that could affect the safety of flight of the helicopter if it is not functioning in accordance with the manufacturers specifications.
- A duplicate safety inspection, as detailed in CAR 43.113, is designed to verify that a critical maintenance task has been done correctly and identify any errors that may have been made during the conduct of the maintenance task. To minimise the risk of an error not being identified, an inspection is completed by another engineer who was not involved in doing the maintenance task. The effectiveness of duplicate inspections has been debated at length within the industry; while they can be fallible, they are generally considered an effective mechanism for trapping errors. Best practice techniques include conducting the independent inspection as soon as possible following the original inspection (United Kingdom Civil Aviation Authority, 2003).
- Despite the requirement for duplicate safety inspections, maintenance error remains a contributing cause to aviation accidents both within New Zealand and globally. Analysis of a 10-year data set of United States helicopter accidents between 2005 and 2015 found a significant clustering of accidents immediately following release from maintenance (Saleh, Tikayat, Zhang, & Churchwell, 2019). Errors during installation and errors associated with visual inspection are amongst the most frequent type of maintenance error (Rashid, Place, & Braithwaite, 2013) (United Kingdom Civil Aviation Authority, 2016). In relation to the 10-year US data set, Saleh et al. (2019) found improper or incomplete (re)assembly or installation of a part accounted for 57% of maintenance errors, followed by 35% failure to perform a required preventative maintenance and inspection task.
- The leading cause of failure to follow maintenance procedures is unintentional error. This includes errors relating to attention and memory, including distractions and interruptions (Key, et al., 2022). During their work on the left hydraulic servo, Engineer A was exposed to at least three distractions, including the interruption by the customer arriving at the hangar, the clean-up of the leaking hydraulic fluid and the trips back and forth to the sonic bath whilst cleaning the sight glass. The maintenance provider had a system in place to manage distraction (this was by the use of a red ribbon that would be hung on the appropriate aircraft location to provide a visible reminder of any unfinished work), however Engineer A considered this only applicable for extended time away from a task (such as taking a lunch break or at the end of the shift). While it is possible the initial distraction of the customer may not have interfered with Engineer A’s ability to return and complete the installation, the additional distraction of the leaking hydraulic fluid increased the amount of interruption time and therefore increased the likelihood that an omission error could be made.
- Despite not completing the installation of the left servo, Engineer A had an opportunity to become aware of this during their write-up of the first part of the duplicate safety inspection. During interviews, Engineer A informed Commission investigators that best practice would be to write up the duplicate safety inspection paperwork immediately after finishing the job. Further best practice would be to include the torque value for the bolts installed during the task in the write-up.
- Another type of unintentional error relates to visual perception, which can contribute to errors in inspection tasks. Engineer B should have discovered that the left-hand servo installation was incomplete as part of the duplicate inspection they performed on Monday 15 July 2024. During Commission interviews, Engineer B was unable to offer any explanation as to why they did not notice the nuts had not been fully tightened to the correct torque or that the missing locking pins had not been installed. Information they were able to provide to Commission investigators indicates that it was possible they became distracted at some point during their walk-around of the left-hand side of the helicopter and never inspected the servo. Alternatively, they did inspect the left-hand side but failed to notice the incomplete installation, effectively looking but not seeing (inattentional blindness).
- Engineer B also informed the Commission that due to personal circumstances they were managing at the time of the event, their normal sleep pattern had become broken. It is therefore likely they were experiencing a level of cumulative fatigue that contributed to the error. While Engineer B had considered themselves fit for duty, in hindsight they considered it possible that their personal circumstances may have led to a degree of preoccupation that increased the likelihood of making an error.
-
It is very likely that the engineers who conducted each part of the duplicate safety inspection were distracted and did not verify that the left servo had been correctly installed.
Post-maintenance acceptance checks
-
The AS 350 BA helicopter flight manual details the checks the pilot is required to undertake prior to flight. The first point in the first section, Exterior Checks, states:
Make sure that all flightworthiness-required corrective maintenance operations have been performed.
- The helicopter flight manual (also known as the Pilot Operating Handbook (POH)) is the primary source of guidance for the pilot operating a helicopter, including the pre-flight checks to be completed.
- While the helicopter flight manual had no specific requirement to check the condition and security of the flight control system, it detailed making sure all corrective maintenance operations had been performed.
- In addition to these checks, as part of the return-to-service process, a check for FOD is completed by another independent engineer prior to the cowls being reinstalled on the helicopter.
-
Prior to being released to service, the helicopter underwent operational flight checks under a limited release to service. This involved three flights to check the main rotor blade track and balance and verify the serviceability of other flight systems. The pilot flew the helicopter for the three main rotor blade track and balance flights.
- On the morning of Saturday 20 July 2024, an operational check flight50 was completed by the operator’s chief pilot and Engineer B to ensure the aircraft was serviceable after the maintenance check.
- The pilot conducted a pre-flight check of the helicopter and then departed with the operator’s chief pilot as a passenger for the flight to Franz Josef.
- Four appropriately trained and qualified individuals inspected the helicopter for airworthiness prior to the accident flight. All were aware that the left and right main rotor hydraulic servos had been swapped during maintenance. Each individual was required, and had the appropriate opportunity, to inspect the helicopter, and each certified that they had done so.
- A thorough handover and pre-flight inspection are important following any maintenance activity, especially for any disturbance of the primary flight controls. They provide another opportunity to identify any maintenance errors and ensure they are rectified before the aircraft is flown.
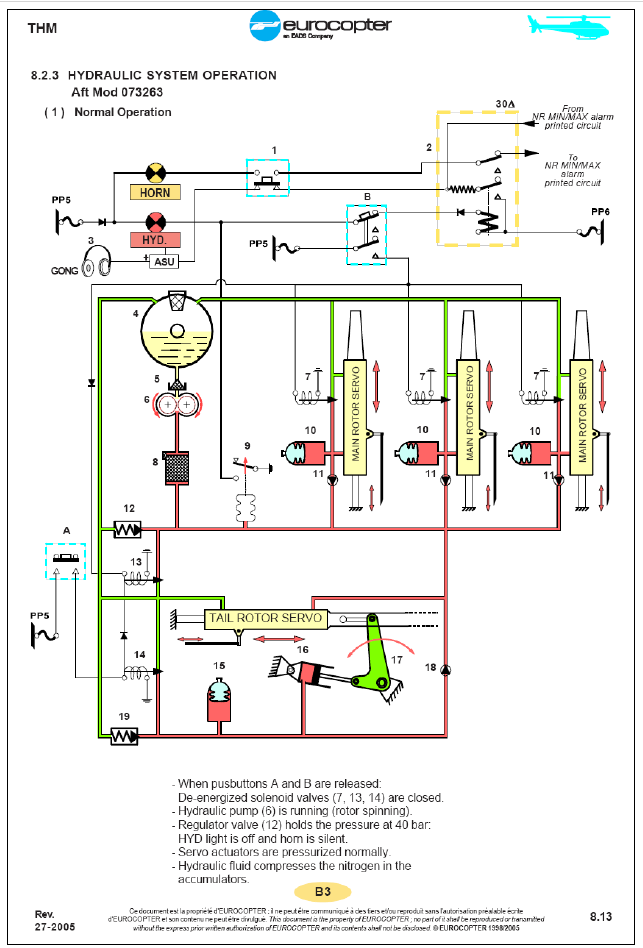
Appendix 1. AS350 Hydraulic System





Appendix 2. Standard Practice Instruction SPI116 – Duplicate Safety Inspection of Controls


Appendix 3. Duplicate Safety Inspection Form